
|
medpundit |
||
|
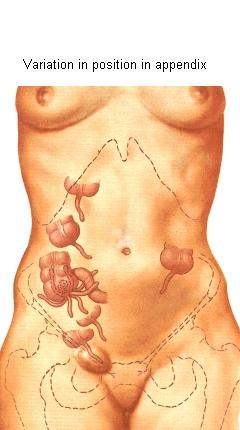
Tuesday, May 06, 2003As it turns out, appendicitis isn’t always as straight forward as it would seem. A textbook case begins as pain around the belly button and progresses to a more localized pain in the right lower abdomen, accompanied by a lack of appetite. Often, there’s also vomiting, constipation, and fever. However, our bodies don’t read the textbooks. The appendix, a worm-like appendage of dubious usefulness, usually hangs straight down from the first portion of the large intestine, the cecum. However, like so many other things biological, the position of the appendix, and of the cecum within the abdominal cavity can vary widely. When an appendix sitting in a “normal” position gets infected and inflamed, it causes the classic textbook symptoms of right lower abdominal pain and tenderness. This, however, only happens about fifty percent of the time. An appendix sitting behind the obturator muscle causes a pain sensation in the pelvis, sometimes only detected with a rectal exam. An appendix behind the psoas muscle causes side pain. Sometimes, it hides behind the cecum, causing only mild pain in response to the doctor’s probing hands on the abdomen. In pregnant women, it gets even harder since the appendix can be displaced just about anywhere and shielded from examination by the enlarged uterus. And, to complicate matters, most abdominal pain does not turn out to be appendicitis. Ovarian cysts, urinary tract infections, gastrointestinal viruses, and kidney stones, to name just a few, can present in a similar manner. And, since surgery is a risky business, doctors only like to operate if the likelihood of appendicitis is fairly high. So, we're constantly searching for something that will increase our diagnostic certainty. Looking for higher numbers of white blood cells in the blood than usual is helpful, but not a certain indicator of appendicitis. Ultrasound can sometimes help to identify an enlarged and inflamed appendix, but it can miss cases, too. The state of the art at the moment is to use helical CT scans when in doubt. They give a high-resolution picture of the appendix that can pick up inflammation in surrounding tissue even at early stages. And, most importantly, they can identify a normal appendix. If diagnosed within the first twenty-four to thirty-six hours, the surgical cure is relatively straightforward and simple. These days, it can be done laparoscopically, which means fewer surgical complications and a faster recovery time. Usually, patients go home the day after surgery if all goes well, leaving their appendices behind them. (Note: For the medically inclined, here’s a good review article on diagnosing appendicitis. And, although written in 1921, you still can’t beat Cope's Early Diagnosis of the Acute Abdomen for a thorough discussion of the nuances of appendicitis.) posted by Sydney on 5/06/2003 07:31:00 AM 0 comments 0 Comments: |

|


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}