"When many cures are offered for a disease, it means the disease is not curable" -Anton Chekhov
''Once you tell people there's a cure for something, the more likely they are to pressure doctors to prescribe it.'' -Robert Ehrlich, drug advertising executive.
"Opinions are like sphincters, everyone has one." - Chris Rangel
Hiatus: I'll be absent for the weekend. Regular blogging will resume on Monday. In the meantime, feel free to browse the archives, (apologies if they aren't working, blogspot's been having problems lately), or any of the fine links to the left. If you're in an Easter mood, don't miss The Passion of Christ in Art. (via Out of Lascaux) posted by Sydney on
4/18/2003 08:40:00 AM
0 comments
Break Through: Texas researchers may have made a groundbreaking discovery in hepatitis C treatment. They've discovered how the virus evades the immune system:
The immune system has many ways to detect and fight off invading microbes, and microbes have just as many ways to elude and disarm immune system components. Through a series of experiments on cells grown in the laboratory, Drs. Gale and Lemon defined the strategy HCV uses to evade the host's immune response. As HCV begins to replicate in its human host, it manufactures enzymes, called proteases, which it requires to transform viral proteins into their functional forms. The Texas investigators determined that one viral protease, NS3/4A, specifically inhibits a key immune system molecule, interferon regulatory factor-3 (IRF-3). IRF-3 orchestrates a range of antiviral responses. Without this master switch, antiviral responses never begin, and HCV can gain a foothold and persist in its host.
Next, the scientists searched for ways to reverse the IRF-3 blockade. They applied a protease inhibitor to human cells containing modified HCV. This prevented the virus from making functional NS3/4A and restored the cells' IRF-3 pathway. Follow-up studies have shown that once restored, the immune response reduced viral levels to nearly undetectable levels within days, according to Dr. Gale.
The identification of this viral protease-regulated control of IRF-3 opens new avenues in both clinical and basic research on hepatitis C, notes Dr. Gale. Until now, scientists had not considered the possibility that inhibiting this protease did anything more than halt viral replication. "Now that we know NS3/4A inhibition essentially restores the host's immune response to the virus, we can assess hepatitis drug candidates for this ability as well," Dr. Gale says.
This is fantastic news. It will lead to a whole new way of thinking about treatment and drug development. Stay tuned.... posted by Sydney on
4/18/2003 08:37:00 AM
0 comments
SARS Roundup: On the reassuring end, there are probably far fewer cases of SARS in the US than previously believed:
About three dozen Americans have probable cases of SARS using the definition of the deadly flu-like disease followed by the rest of the world, federal officials said Thursday.
In all, the Centers for Disease Control and Prevention lists 208 Americans from 34 states as probable or suspected SARS cases. However, only 35 of them meet the definition for probable cases of the disease set by the World Health Organization.
CDC Director Dr. Julie Gerberding said the agency will begin using the WHO definition because ``we don't want to exaggerate the scope of the problem here by including patients'' who would not be considered SARS cases elsewhere.
Many of the suspected U.S. cases had only mild flulike symptoms, and less than one-quarter were hospitalized. Most were on the list because of recent travel to a part of the world with SARS.
Having a test to diagnose it accurately will certainly help paint a better picture of the virus’s natural history and true mortality. The CDC version of a diagnostic test might be available as early as next week:
One version created by the Centers for Disease Control and Prevention could be shipped to state labs as soon as the end of next week, officials say. Several others are being fine tuned around the world using new information compiled just last weekend from scientists' marathon exercise of decoding the virus's genes.
The tests, which search for viral genes in victims' nasal secretions and other samples, are likely to work only in the early stages of the disease, before the body defeats the virus, removing all traces it existed.
They will be used cautiously at first, while developers work to prove they pinpoint the virus in infected people without sending up frequent false alarms in the healthy. Until this accuracy is known, "we will be loath to say someone doesn't have SARS on the basis of the test," CDC head Dr. Julie Gerberding said Thursday.
Two doctors from Hong Kong document their experience with SARS:
The disease, initially affecting mainly healthcare workers, spread rapidly to the community as family members became infected and in turn infected their coworkers and friends. When symptoms developed, they consulted their general practitioners, leading to more healthcare workers developing the disease.
Although one would hope that hospitals would see in this pattern of infection the potential for harm in the event of a smallpox attack, The Bloviator points to evidence that they’re taking home the wrong lesson. Instead of offering pre-attack smallpox vaccination to their employees, at least two hospitals say they would turn away potential smallpox victims instead:
St. Vincent's Hospital, a 758-bed acute-care facility in Manhattan, recently held a drill to prepare for a nuclear, biological or chemical terrorist attack. The first step: Lock down the hospital so that no new patients could come in.
"If we can't protect the people who are here, we can't do our job," says Richard Westfal, assistant director of emergency medicine at St. Vincent's.....
In Houston, St. Luke's Episcopal Hospital is vaccinating up to 75 of its staffers against the smallpox virus. But since smallpox doesn't have a cure and kills about 30% of its victims, hospital officials say they would lock down the moment conditions were deemed unsafe for those within.
Such a policy "may not have the needs of the [smallpox] victims in mind," says Herbert DuPont, chief of internal medicine at St. Luke's, but he says St. Luke's first priority should be to its patients, staff and their families.
Of course, if they offered the vaccine to more than 75 staff members, they wouldn’t have to shut down. (RangelMD agrees with me that our public health officials should be paying attention to SARS as an example of the importance of acting now, via preattack vaccination, to prevent a potentially far worse catastrophe with smallpox.) posted by Sydney on
4/18/2003 08:29:00 AM
0 comments
Reading List: The President's Council on Bioethics has published a list of literature to stimulate thought on the issues of modern medical science. It's a diverse list, with selections ranging from the Book of Job to Peter Pan. There will be those who mock it as silly, but there's something reassuring about a bioethics council that considers the humanity behind (and beyond) the science. (via the OpinionJournal) posted by Sydney on
4/18/2003 08:26:00 AM
0 comments
Wrongful Life: A court in the Netherlands has awarded damages to a disabled child on the grounds she should never have been born. Her parents say they would have aborted her if their midwife had done prenatal testing and detected the chromosal abnormality responsible for her disability. But a professor of law points out the problem with this line of thinking:
Joseph Hubben, professor of health law at the Free University of Amsterdam, said: "To recognise a disabled life as a source of financial damages gives the wrong signal to society. Disabled people should be fellow citizens not someone who should have been aborted."
Rebellion: New Yorkers are giving the Bronx cheer to the new anti-smoking laws:
Welcome to civil disobedience, circa 2003. On a beautiful Downtown day this week, Gotham Gandhis in Prada flicked their ash at the mayor from sidewalk cafes and Irish pubs. Everywhere you turned, smoke wisped out beneath spring caps, leaving clouds over the Vespas on West Broadway. Some restaurants have plans to ignore the ban altogether and pass the hat around for the fines. Already, those that do so are packed as if Puff Daddy has just showed up.
I don't condone smoking in any way, but medical advice never works well when it's given punitively. posted by Sydney on
4/17/2003 08:39:00 AM
0 comments
SARS Update: Canadian health officials have been noticing more community-aquired cases of the disease:
Health-care professionals had been looking for people who had recently returned from Southeast Asia, people who had contact with a SARS patient or people who had been at one of two hospitals where uncontained outbreaks occurred. Later, people who had attended an April 3 wake for a man who died of SARS were added to the list.
With word earlier this week that at least 30 members of a Catholic church group had become infected, those trying to contain the spread realized the profile is no longer a tool hospitals can rely on to identify incoming SARS patients.
"We've now seen patients, people coming down in a very close-knit (religious) community," said Low. "We know the potential for secondary transmission is quite high. For every person who has the disease in the community, the potential of exposing who knows how many others and many of those will come down with infections."
It’s enough of a problem that the Catholic church is suspending some rituals, both ordinary and Easter-types:
- The sharing of communion wine.
- Shaking hands or hugging during the sign of peace at masses.
- Kissing the crucifix, known as the veneration of the cross.
- The distribution of communion wafers on parishioners' tongues.
Restrictions on the distribution of communion and handshakes will continue for the duration of the SARS outbreak, Fabbro said in his letter.
What I want to know is, will they move to those little shot-glasses so common in Protestant churches?
A reader wonders if there might not be a lot more SARS cases out there:
The question that came up for me reading your information about SARS has to do with numbers of cases. How do we know what the number of cases actually is? I assume that the cases that get diagnosed are the ones that are serious enough for the people to come to the doctor. In other words, we really only know about that serious cases. Unless, someone goes through the population and tests some sample, we really have no clue as to the infection rate, do we?
That’s true, we don’t have a good handle on the actual infection rate. There could be a lot of milder cases running around that are never diagnosed. Although, once the disease was recognized as a problem in southeast Asia, travellers returning from there were given cards describing the symptoms and advising them to seek treatment if they developed them, so it might not be as widespread as it could be. On the other hand, now that it’s starting to gain a footing in some communities, it’ll be hard to continue to track that, unless a diagnostic test is developed.
That test may be available by Monday in Singapore:
Developed by the government-run Genome Institute of Singapore, the test may be sensitive enough to detect the virus in its early stages before a person develops symptoms such as high fever and a dry cough, the pro-government newspaper said.
"The test has been able to pick up clearly the virus in the blood," Dr Ren Ee Chee, deputy director of the institute, was quoted by the newspaper as saying.
The Centers for Disease Control and Prevention in the United States is working to license and distribute a quick test for the virus, so doctors can tell which patients have SARS as opposed to some other form of pneumonia.
On Monday, a German company, Hamburg-based Artus GmbH, said it was distributing a quick "real-time" test that can detect the virus by looking for its genetic signature.
Ren said the Singapore test was in its final stage of completion.
For Want of an Amino Acid: The very rare disorder, Hutchinson-Gilford progeria, which makes children grow old before their time, is caused by just one amino acid misplacement:
The disease was first identified in 1886, but Brown said it has been difficult to study because "there are only a handful or so alive at one time." He said about one patient with progeria is born each year in the United States.
Collins and his co-authors found the mutation on a gene called lamin A in DNA specimens from 18 of 20 progeria patients. A similar study, appearing in the journal Science, found the gene mutation in two progeria patients.
Collins said that disease is not genetically inherited but develops in each patient. He said there is a suggestion that the progeria gene is transferred to the embryo through a flaw in the genes of the father's sperm.
The flaw, he said, was a substitution of single DNA base. The amino acid guanine is switched to adenine.
Canfield and Lanphear's team studied 172 children in the Rochester, N.Y., area, measuring blood lead levels at ages 6, 12, 18, 24, 36, 48 and 60 months. The children were tested for IQ at both 3 and 5 years of age.
They found that a rise in lead levels from 1 mcg/dl to 10 was associated with a 7.4-point drop in IQ. An increase in lead levels from 10 to 30 mcg/dl was associated with an additional drop of only about two to three IQ points, in line with previous studies....
"People have been asking, `How low (a lead concentration) is low enough?"' said Dr. Richard Canfield of Cornell University, one of the leaders of the study. "The fact is, in our study, we found no evidence for a safe level. There is no safe level of exposure."
The study shows no such thing. The researchers used the Stanford-Binet IQ test to assess the intelligence of three and five year olds. The test, although designed to be used from age two on up, is less accurate in preschool children. But, even more damning are the data themselves. The paper includes a graph (subscription required) of IQ’s against lead levels. The distribution is by no means linear, especially at lead levels less than 10 micrograms/deciliter, the current cut off for lead toxicity. IQ’s at the lowest levels of lead exposure (i.e. under 10micrograms/dl) range from the high 60’s to around 130, with a very widely dispersed distribution of plotted points between. Children with lead levels higher than ten, however, have a much narrower spread of IQ values. The plotted data points for levels below 10 micrograms/dl look more like a globule than a line. Looking at the graph, it’s clear that there’s no association between low lead levels and IQ. But, the researchers use averages to condense it into a nice downward sloping line to prove their hypothesis. It’s a shameful misuse of statistics, especially when you consider that the estimated cost of making all houses absolutely lead free is $32 billion. posted by Sydney on
4/17/2003 07:44:00 AM
0 comments
Apologies: Sorry about the quiz posted on April 15 - I didn't realize the answer required a subscription. The answer: mercury embolism. The patient had injected herself intravenously with elemental mercury. Survived with no ill effects. posted by Sydney on
4/17/2003 07:12:00 AM
0 comments
SARS Update: U.S. healthcare worker unions are getting skittish about SARS:
U.S. health-care workers, edgy over the contagious and sometimes fatal respiratory illness SARS, are pushing U.S. regulators to require isolation rooms and other safeguards to give hospital employees better protection from exposure to infected patients.
It should be noted that SARS has not reached epidemic proportions here in the United States, and that most, if not all, hospitals have isolation rooms and other safeguards against infectious diseases. Perhaps they’re just being prudent. Yet, at the same time, the healthcare worker unions have discouraged their members from getting a vaccine that would protect against a similarly contagious, and far more deadly, infectious disease - smallpox. Do you suppose the SARS experience will change their minds?
Meanwhile...back in parts of the world that have a real SARS problem, characteristics of the clinical course are starting to fall in place:
Data available to WHO indicate that 96% of persons developing SARS recover spontaneously. The focus now is on the roughly 4% who are dying. WHO will hold a clinical teleconference on Wednesday to gather international experiences in the management of SARS patients and pool data on the results of various therapeutic regimens.
That's reassuring. And so is this: the New England Journal of Medicine'sdaily graph (scroll down below the article links) shows the mortality rate remaining flat, even as the numbers of cases skyrocket.
International health officials visited two secretive military hospitals in Beijing to check for unreported cases of severe acute respiratory syndrome, and met with officials from a third, a team spokesman said Tuesday.
The city's military hospitals are rumored to have unreported cases of the fatal disease and such visits are a priority for the World Health Organization team, which is examining how health authorities in the Chinese capital are handling SARS, team spokesman James Palmer said.
I was skeptical of the bioweapon theory of SARS, but I'm beginning to think it more and more likely that it could have been an accidental release of a work in progress...
World Health Organization investigators said Wednesday that China has previously unreported cases of the deadly SARS virus in military hospitals in Beijing and has barred release of details about them.
The investigators who visited two military hospitals in Beijing said they saw SARS patients there and received data on new cases. But they wouldn't say how many patients there were, and said Chinese officials had told them not to release other information. posted by Sydney on
4/16/2003 07:41:00 AM
0 comments
It's All Clear Now: The author of the bible of medical physiology, Dr. Arthur Guyton, died this week. Reading his obituary, I suddenly understand why the book belabored the physiology of hypertension so much:
Dr. Guyton helped clarify the workings of the cardiovascular system through his research into the causes of high blood pressure. In the 1950's, he overturned the conventional wisdom that the heart controlled the amount of blood pumped, demonstrating that cardiac output is instead determined by body tissues' need for oxygen.
In 1966, he used a computer model to establish that the kidneys are the important long-term controllers of blood pressure and that other systems regulate pressure only over the short term.
I don’t exaggerate when I say that the only thing I remember from that text book is the graphic repeated again and again of cardiac output in relation to just about every physiological parameter you can think of. If I close my eyes I can see the graphs just as clearly as if the book were in front of me.
Dr. Guyton was also the father of ten physicians. I always wonder about families in which all the kids go into the same profession. What do you suppose it is that motivates them? I’ve got to think it’s parental pressure, especially when as many as ten kids do it. Surely, those ten kids are different enough to have separate interests and goals. There are a lot of families like this in medicine (and law, too). When interviewed in newspapers they always deny parental pressure, but I always wonder if they’re afraid of offending a very strong parent. The obituary backs this up:
When asked why all of the Guyton children had decided to go into medicine, David, the eldest, said, "Daddy never lectured us about medicine: He stimulated our interest."
Thomas, the ninth child, said, "He instilled the work ethic in all of us, but I think I learned most from his disability." [ed. note - The obituary never clarifies what that disability was - workaholic, perhaps?]
There were, of course, other motivating factors.
In a 1993 article in Harvard Magazine celebrating his father's 50th reunion and the graduation of his youngest sibling from medical school, Douglas, the seventh child, admitted: "The pressure on me was intense. I can only imagine what it must have been like for the three youngest."
Which brings me to one of my favorite medical family stories. When Waldo Nelson, the author of the bible of pediatrics , Nelson's Textbook of Pediatrics, died a few years ago, the New York Times obituary noted that when he was putting together the the first edition, he made it a family affair. His wife and kids were given the job of putting the index together. One of his teenage daughters slipped this entry in:
Birds, for the .... pp.1-1,413
It made it past both her father and the proof readers and into print. Kids! posted by Sydney on
4/16/2003 07:32:00 AM
0 comments
Dang: Another illusion shattered. Derek Lowe says that those silicon-based lifeforms from science fiction are bogus. He also has a good post on ribaviran and SARS just below it. posted by Sydney on
4/16/2003 07:30:00 AM
0 comments
Tuesday, April 15, 2003
Quiz: Guess the diagnosis. (Hint: Dental assistant who attempted suicide.) Answer.
APOLOGIES: I thought that the link to the answer was one of the New England Journal's free pages, but it turns out it requires a subscription. Answer: Mercury embolism. She injected herself with elemental mercury. Survived with no ill effects. posted by Sydney on
4/15/2003 08:26:00 AM
0 comments
Linus Pauling Syndrome: Dr. Henry Heimlich, renowned for the famous Heimlich maneuver, is making waves with a controversial AIDS therapy. He plans to deliberately infect AIDS patients with malaria to see if it cures their AIDS. What do sane people think?
"This comes up periodically, but malaria has never worked for anything...If Heimlich is really doing this, he should be put in jail," said Mark Harrington, executive director of Treatment Action Group, an AIDS research advocacy organisation.
Dr. Heimlich says there is reason to think his method will work, and is not a danger to the already immunosuppressed AIDS patients. The CDC says otherwise:
In 1993, the U.S. Centres for Disease Control and Prevention issued a memorandum saying malarial therapy could not be justified because it might well do more harm than good.
He already did a preliminary trial in China, and his collaborators are now in trouble:
Meanwhile the University of California at Los Angeles is investigating whether two of its medical researchers took part in the Chinese malarial therapy trial. The university said a medical review board is looking into whether Dr John Fahey and Dr Najib Aziz violated policies that regulate tests on humans. On February 16, the Cincinnati Enquirer published an article in which Heimlich described his work in China and said Fahey was involved.
"He is a fine person who gave of himself and helped tremendously. It is exceedingly reprehensible for him to be challenged in this way," Heimlich said.
Some might say it’s exceedingly reprehensible to deliberately infect someone with a bad immune system with a disease that can itself be deadly - and one that is increasingly resistant to antibiotic therapy. The fact that the research is being done in the Third World, which doesn’t have the same patient-protection laws that the developed world has, speaks volumes. posted by Sydney on
4/15/2003 08:24:00 AM
0 comments
Medical Ethics: Perhaps a part of me remains hopelessly idealistic and naive, but I find this shocking:
He could have been a fedayeen fighter. Or a thief. Or he could have been just an innocent man who panicked. But the angry crowd of mostly Arab hospital workers had made up its mind.
"Who is he?" someone asked as the man's bullet-riddled body was wheeled toward the emergency room door.
"This is a criminal who wanted to kill us!" shouted one of the hospital workers, who then spit on the wounded man as hospital workers cheered.
"Kurds are coming to rob and kill us, so we kill them," said another, who also spat on the man.
A third hospital worker kicked the man in the head. Then the hospital's staff blocked the door with their bodies and refused to treat him.
"Kurdish are criminals," one Arab staff member said....
People in the crowd outside the hospital assumed the two prisoners were looters, and nearly set upon them. But an American Special Forces soldier drew a pistol and repeatedly screamed at the crowd to get back. Once he moved the wounded prisoner inside the hospital, a doctor refused to treat him.
"He's shot!" the Green Berets soldier shouted at a physician. "You're a doctor. It's your job to look at him."
That soldier has a better understanding of medical ethics than the hosptial staff and doctor. Amazing. Is it any wonder people have been looting hospitals? They probably feel safer taking medical matters in their own hands. At least they’d avoid a kick in the head. posted by Sydney on
4/15/2003 08:01:00 AM
0 comments
Go Ask Alice:Dr. Alice is on a roll this week - the pain of HIPAA, Grand Rounds translations, and shocking Hungarian dance cards. posted by Sydney on
4/15/2003 07:55:00 AM
0 comments
Computer Medicine:RangelMD has some good advice for those seeking to build a better electronic medical record system. posted by Sydney on
4/15/2003 07:54:00 AM
0 comments
The bill approved today sets up no-fault compensation, to be financed this year with $42 million from an Iraq war spending measure. Permanently disabled recipients would be eligible for up to $50,000 a year in lost wages. Partly disabled recipients would collect also that benefit, up to a maximum of $262,000. The government would pay a $262,000 benefit to spouses of people killed by the vaccinations. Spouses with children would be eligible for either $262,000 or $50,000 a year until the children turn 18.
Now, here’s the million dollar question. Will the compensation be limited to those suffering known side effects and complications of the vaccination, or will it include those coincidental illnesses like gallbladder disease and heart attacks? posted by Sydney on
4/15/2003 07:53:00 AM
0 comments
FDA Scrutiny: The FDA is reviewing a possible link between the newer, safer, antipsychotics and diabetes(requires subscription):
Of the millions of patients who took the drug over an eight-year period that ended in 2002, 288 are reported to have developed diabetes.
Seventy-five of those people became severely ill, and 23 died. Some researchers see these statistics as significant because in some cases diabetes symptoms came on suddenly after patients began taking Zyprexa, eased after they went off the drug and returned when they tried the medication again.
288 out of millions is hardly proof of an association, ( click here for more on the subject), and one would hope that the FDA doesn’t use this as a reason to remove the drugs from the market. They are much more effective and safer than older drugs for schizophrenics, which have their own special toxicities at much higher rates than 288 per millions. But, a warning that monitoring blood sugar levels when someone is first placed on the drug isn’t a bad idea. It could be that the drug unmasks diabetes earlier in some people, much the way that pregnancy does. posted by Sydney on
4/15/2003 07:46:00 AM
0 comments
Scientists in Canada announced over the weekend that they had broken the genetic code of the virus suspected of causing severe acute respiratory syndrome.
Sequencing the genome -- which computers at the British Columbia Cancer Agency in Vancouver completed at 4 a.m. Saturday after a team slaved over the problem 24 hours a day for a mere six days -- is the first step toward developing a diagnostic test for the SARS virus, and possibly a vaccine.
Amazingly quick work. Like Dr. McCoy in Star Trek. And it appears to be unrelated to any other known coronavirus:
Canadian researchers said the genome appears to be that of a "completely new" coronavirus unrelated to any known human or animal viruses.
That may make it harder to control. If it had been related to an animal virus, controlling human exposure to the animal of origin would help to contain the spread of the disease. Makes you wonder where it came from. A lab?
ADDENDUM: I don't mean to imply that the SARS coronavirus is a bioweapon. It could have been accidently introduced from a lab doing genetic manipulation on viruses. The reasons for that sort of work could be benign - or not. posted by Sydney on
4/14/2003 01:08:00 PM
0 comments
California Punitive Medicine: California is suing restaurants for selling fish:
Lawsuits filed Thursday in Los Angeles and San Francisco superior courts claim that restaurants such as Morton's, Ruth's Chris Steak House and Benihana, were not following Proposition 65 guidelines. The guidelines require businesses to post warnings when they expose people to carcinogens.
The lawsuits claim the restaurants serve fresh or frozen swordfish, tuna or shark, which contain enough mercury compounds to trigger the law's provisions. The state is seeking an injunction requiring the restaurants to post warnings, as well as civil penalties of $2,500 per day for each violation.
Other affected chains are Red Lobster and Olive Garden (Darden Restaurants); Chili's, Macaroni Grill and Little Italy (Brinker International); Outback and Roy's (Outback); Chart House (Landry's Restaurants); Bennigan's (Metromedia Restaurant Group); Cheesecake Factory; Hof's Hut; Claim Jumper; and P.F. Chang's China Bistro.
Has anyone ever seen a case of clinical mercury poisoning from eating fish at a restaurant? Has anyone in the United States seen a case of clinical mercury poisoning that wasn’t related to occupational exposure? I couldn’t find any.
"Certainly mercury is an issue," said Greg Ochinero, board member of the California Restaurant Association's Silicon Valley Chapter. "But ... I can't imagine why the blame would be laid upon the restaurant industry. They aren't the ones that cause the pollution that puts the mercury in the food in the first place." posted by Sydney on
4/14/2003 08:06:00 AM
0 comments
Punitive Medicine II: Although commenting on public health medicine’s inclination to expand the definition of disease to include social problems that are better handled by law enforcement (domestic violence, or any violence, for that matter) or the conventions of polite society (smoking), causes a bad case of the vapors in some people, episodes like this one in Italy illustrate just how this approach quickly turns public health medicine into punitive medicine:
Despite being a non-smoker with smoke sensitive eyes, I am strongly opposed to the new restrictions on smokers. At least once a week, my wife and I take our two-year-old son and four-month-old baby to eat out in restaurants in Italy and we encounter smokers. But like most people, I am perfectly capable of asking people near us not to smoke.
In these situations, the Italian health minister advises, "call the police." In the city of Trento patients recently did exactly that after a physician refused to stop smoking in a hospital waiting room. He was fined and reported to the national health service. Are we really so pathetic that we need the intervention of the health police?
No doubt, that physician was being very rude. But, what do you suppose motivated his rudeness? Was it a total disregard for those around him, or a rebellion against the draconian smoking laws? Remember Prohibition, and all the violence it bred? Well, look what happened this weekend in New York. It isn’t a stretch to say that people are beginning to feel needlessly put upon by these stringent anti-smoking laws. Wouldn’t it make more sense to provide a separate smoking room in public places than to ban it all together? posted by Sydney on
4/14/2003 08:00:00 AM
0 comments
Vietnam Syndrome: A reader pointed out that my Tech Central Station article on military medicine’s contribution to peacetime medical advancements neglected the Vietnam War:
I will probably not be the only former "Special Operations Medic" to let you know that we were doing all of this, as well a fair amount of not-so-minor surgery, in the Vietnam War. In fact, Special Forces medics in the 1960's could intubate, insert chest tubes, do venous cut-downs, and insert central lines when necessary- in the field. I have repaired hand tendons in the field, completed traumatic amputations, done fasciotomies for burns, delivered babies, done myringotomy- not "minor" procedures. ("There is no 'minor' surgery, only minor surgeons", as I recall being told many times in training).
We also did a fair amount and a wide variety of lab work, primarily concerned with diagnosis of tropical disease (thick and thin smears for malaria, identification of the huge variety of parasites- a couple of which I managed to contract- Gram stains, AFB's for TB, etc etc.)We had quite a good lab kit, including microscope, centrifuge, and a number of stains that was packaged so as to be parachutable. We also did a lot of preventive medicine, some Pediatrics (treating local village children), and even dentistry (primarily extractions) and Veterinary medicine, farm animals being extremely important to the people we worked with in Southeast Asia. To serve on a "A" Team required a minimum of three Military Occupational Specialties , chosen from a list of five at that time (Medical / Weapons / Demolitions / Operations and Intelligence / Communications). I was trained in, and taught, Light Weapons and Demolitions, in addition to my duties as a Medic. Although Special Forces Medics carried Geneva Convention cards, it is highly doubtful that we were really entitled to the protections afforded full-time medical personnel...
I have been a P.A. since 1976, and I realized early in P.A. training (Baylor) that we S.F. Medics knew practically nothing about Internal Medicine, aside from tropical infectious diseases. Most of my P.A. class, by the way, were former Special Forces Medics. But we DID know trauma. In fact, I was struck, when I took the ATLS course for the first time in 1983, by just how closely it followed the protocols of the old Special Forces "Dog Lab" at Fort Bragg. And the emphasis on rapid decision-making and fast, effective interventions was precisely the same. (The dogs in the dog lab have long since been replaced by goats- apparently few people grow misty-eyed over a wounded goat.)
I would also expand on your theme, that war brings rapid medical advancement. I recall the haphazard ambulance services of the 1950's and 1960's clearly- they were basically "scoop-and-run" operations, with little to no capability for lifesaving interventions en route. I grew up in Manhattan, and once in awhile an intern would be sent out with an ambulance, to do what he or she could with what was in their little black bag. Generally, however, ambulance attendants were poorly-paid hospital aides, or drivers with zero medical training.
The experience of the Vietnam War changed that, as highly-trained military Physicians and medics returned home, and put the lessons of triage, forward lifesaving treatment, and advanced trauma training for ambulance attendants into practice across the country. Of course, this was the genesis of the whole EMT/ Paramedic system that we have today, which saves many thousands of lives a year. I include aeromedical evacuation as part of this system. Would this evolution have occurred without the war? Probably- but at a very much slower pace, and with many experimental approaches (some of which would probably have been disasters). As it happened, the military brought the system to a high level of efficiency, and then it was further refined by expert trauma surgeons, ER staff, and others back in the U.S.
Much of this history has been forgotten, or deliberately neglected. Many of the Physicians who wound up training and working with EMT's and Paramedics had not been to war, and were very dismissive of any possibility that military training could be useful in the civilian environment. And the country REALLY wanted to forget the Vietnam experience- so those with military backgrounds did not advertise the fact in their new, civilian occupations. There is an almost complete lack of appreciation for the tremendous strides brought about in emergency treatment of patients at accident scenes, etc, which we owe to the military.
He’s right. I didn’t notice it at the time, but all of the sources I used to research the past contributions of wars to medical technology neglected the Vietnam War. I went back and looked at the book that inspired that article, Combat Surgeons by John Laffin, and its description of the Vietnam War is only one of lament - of the horrible conditions that medics and surgeons had to face and the terrible toll it took on them. There was one thing, though, that stood out in his description of combat medicine in Vietnam - the Vietcong would deliberately shoot to wound the scout who walked ahead of a line of soldiers. They knew that he would call for the medic, then when the medic came running, they would shoot to kill the medic. They figured they’d do far more harm to the platoon that way than just shooting the scout. It’s a tremendous credit to the bravery of the medics that they always came running when called. posted by Sydney on
4/14/2003 07:38:00 AM
0 comments
Sunday, April 13, 2003
Medpundit Art History Lesson: Europe in 1830 was not a restful place. It was a peaceful place for the first time in centuries, but it was not restful, for the peace came at a great price. The powers of Europe, the monarchs who had so recently been sent running by Napoleon, were determined that those liberal “French ideas” of liberty and republicanism would be stamped out forever, and they united in their purpose to see that this happened. Ruling families who had fought viciously among one another before Napoleon, now were united for the first time in history in a common goal. They would aid one another against the usurpation of the common man. This European alliance enforced the peace with secret police and harsh punishment for anyone who dared to breathe a word of the rights of man. But even a people exhausted by endless war can only stand so much repression, and in July of that year things came to a head in - where else? - France.
The last of the Bourbon kings, Charles X, had as his primary political goal, the re-establishment of the ancien regime - the monarchy as it had been before the first French Revolution. He strengthened the power of the clergy, restricted voting rights, silenced the press, and disbanded a newly elected liberal cabinet. The people’s response was swift and violent. The July Revolution lasted only a few days, but by its end, Charles X and his ministers were gone, and the liberal ideals of the first French Republic stirred to life once again across all of Europe.
One of those standing and fighting (or at least observing) on the barricades of Paris that July was the Romantic painter, Eugene Delacroix (1798 - 1863), an event he commemorated by painting, Liberty Leading the People.
In it, we see Liberty portrayed with all the accoutrements of the first French Republic. She wears the breast-exposing dress so fashionable in the early days of the First Republic and the revolutionary Phrygian cap, which was not only the headware of choice of freed Roman slaves, but is also a term used in medicine to describe an anatomical variant of the gallbladder. Above her head she hoists the Tricolour. There’s nothing pretty about the scene. The people following Liberty can only be described as a mob, brandishing their swords,spikes, and guns with wanton disregard for safety. Even the young are not immune to the frenzy, as demonstrated by the pistol-toting boy at Liberty’s side. In the background, in a smokey haze, stands Paris. Liberty carries in her hand, a gun, and beneath her feet lie the dead of the current regime, one of whom is ingloriously stripped of his trousers. The message is clear - Liberty comes at a price. It is not a gift that rulers give freely to the ruled, but a gift that must be fought for, and protected, no matter what the cost. The painting hung in the palace of Louis Philippe, the "Citizen-King" who replaced Charles X to remind him that his power came from the people, not from divine right. At least it hung there until he tired of being reminded of that fact and took it down. Not surprisingly, his fate was also to be dethroned by a revolution.
Some art historians consider this the first political work of modern painting. If so, it’s fitting that it should have been painted by Delacroix. For, although his true parentage was the subject of considerable gossip, there’s no doubt that his was a political heritage. His father of record was Charles Delacroix, the foreign minister in the first French Republic, until he was replaced by Talleyrand. Eugene was born after Charles had a highly publicized surgery to correct a testicular deformity. Gossip had it that Talleyrand replaced him in more than just political office, for Eugene Delacroix bore more of a resemblance to the master politician than he did to Charles Delacroix.
The artist was himself a political animal, a member of the French National Guard, and agitator for the ideals of liberty and republicanism. He painted himself into his portrayal of Liberty Leading the People. That's him, directly behind Liberty, wearing a top hat and carrying a gun.
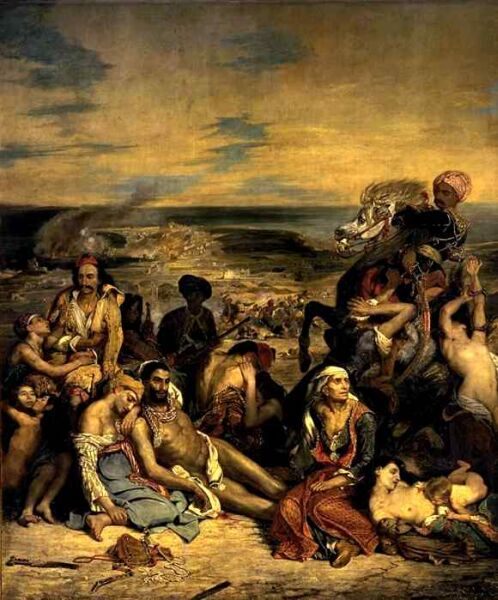
Delacroix was in the vanguard of the Romantic movement. He eschewed the clean, sober, idealized work of the previous generation of neoclassicists, for the gaudy, dramatic imagery of the neo-Baroque. Some found his style so offensive that they described his Salon piece, Massacre at Chios, as the “massacre of painting.” But it was the dawning of a new age, both in art and in politics, and his style soon became the accepted art form throughout all of Europe. By the time of his death from tuberculosis in 1863, he had completed 1,000 paintings, 2,000 watercolors, and 9,000 drawings. Prodigious by any standard. posted by Sydney on
4/13/2003 08:40:00 PM
0 comments
Appropriate: On a Palm Sunday note: some Iraqis were waving palm fronds in celebration last week. (It’s still a tradition of celebration in the Middle East.) posted by Sydney on
4/13/2003 09:00:00 AM
0 comments





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}