"When many cures are offered for a disease, it means the disease is not curable" -Anton Chekhov
''Once you tell people there's a cure for something, the more likely they are to pressure doctors to prescribe it.'' -Robert Ehrlich, drug advertising executive.
"Opinions are like sphincters, everyone has one." - Chris Rangel
Trust Me, I'm a Doctor: Writing on NRO, James Lacy says that there's little evidence of civilian casualties in Iraqi hospitals, despite what doctors tell reporters:
I asked the only female doctor present how many patients they had treated who had been injured in the fighting, and how many of them were men. She replied that they had treated about 600 patients and that they were mostly men. Dr. Ali quickly corrected her and they began to argue in Arabic. He then announced that it had been about half men and half women.
Dr. Ali insisted on being my escort for the remainder of the visit. He explained that the hospital's fifth and sixth floors were reserved for civilians who had been injured in the war. Men were on the sixth floor, women and children on the floor below.
The first room off the elevator was filled with the men who had suffered the worst injuries. None of them spoke as the doctor showed me each of their many wounds.
I went from room to room without saying a word. It was hard to look at the broken bodies lying in such unsanitary conditions, but I also noticed something else. There was only one man who seemed to be over age 40 on the entire floor. Of the 46 patients I counted, 45 appeared to be in their early twenties.
When I visited the women's and children's floor, most of the rooms were empty. Besides Esraa and Nor, there was only one middle-aged woman, who had been wounded in the side by shrapnel. She also was expected to make a full recovery.
I asked Dr. Ali why, if these were all civilian casualties, there was not an even distribution of males and females and among age groups. Why did the overwhelming number of them appear to be men of military age? He offered no explanation, but continued to insist that the men were all civilians. He then added that many civilians had been killed, too, and I should check the morgue and see.
When I did try to check the morgue, they would not allow me to see any of the wrapped bodies, but did let me go through the paperwork. At my request, a clerk pointed out where the name was supposed to be on each form. Most of the name blocks were blank. Pressed for an explanation he said, "They are not known here." It was only then that it struck me that most of the men lying in the hospital had no family around them — unlike Esraa and Nor, who were surrounded by family members. The clerk's statement probably meant that these men were fighters from Baghdad, who had no relatives in Najaf.
It should come as no surprise that Iraqi doctors are prone to exaggerating the extent of American-caused casualties. In a totalitarian regime, those people who embrace the party-line are the ones who get ahead. This is true in all walks of life, not just politics. And it's especially true in fields that require an education in state schools. This happened in Nazi Germany, too. So why aren't reporters more skeptical of Iraqis in positions of authority? Especially after they've witnessed scenes like this?
Turns out things aren’t so bad in Baghdad, either :
There are more hospital beds available in Baghdad than there are patients to fill them, the U.S. officials said late last week.
The International Committee of the Red Cross provided some independent backing for that claim, reporting that the 250-bed Al Na'uman hospital had 90 patients.
"The staff are generally less busy now, and carry out five to six surgical interventions a day," the report said.
...Doctors at two Baghdad hospitals — one state-run and the other private — said in interviews that their main business was attending to people with gunshot wounds or burns caused by antilooter and antitheft vigilante activities, score-settling, handling of unexploded ordnance and general lawlessness.
..."The unfortunate part, the problem we have, is we continue to get these offers and donations that really overwhelm the system," she said.
"Drugs and medications get outdated. The amount is just too much," she added. "We have enough crutches and bandages to last us 10 years."
...The most important medical need in Iraq now, officials said, is to vaccinate children younger than 5. One in three Iraqi children of that age has not been immunized, whereas almost all children of the same age in neighboring states have had the vaccinations
If they have the time and energy to turn their attention to preventive medicine, then things can't be all that bad. And notice that those children haven't been immunized in the past five years. Just what were they doing before the fall of Baghdad? It suggests that the state of medicine may actually be improving in Iraq since the liberation, rather than declining.
posted by Sydney on
5/07/2003 08:00:00 AM
0 comments
Medicine in the Anglosphere: A recent survey within the Anglosphere shows that a quarter of patients have experienced medical errors:
The Harvard survey of sick adults was conducted in the United States, Canada, the United Kingdom, Australia and New Zealand. At least 750 persons were surveyed in each country.
The United States had the highest portion reporting errors -- 28 percent -- and the United Kingdom the fewest, 18 percent. But in all five countries, those who went to more than two doctors complained of errors almost twice as much as those who went to just one or two physicians.
...''This is only 10 percent of patients,'' he said, ``but they're an expensive 10 percent.''
The survey showed that more than one in four -- 28 percent -- of those who see more than two doctors in the United States and Canada said they were given duplicate tests by different doctors. And roughly a quarter in all five countries said they received conflicting information from different doctors.
One of the experts interviewed in the article suggests that paying for “case managers” to coordinate care would help prevent these sort of errors. You know, there are people out there who do this now. They’re called primary care physicians.
But Florida has come up with unique plan to reduce medical errors:
Last week, the Florida Legislature, attempting to cut down on medical errors, passed a bill ordering doctors to improve their handwriting, so that pharmacists and nurses could do a better job of reading prescriptions.
Payouts: The crux of the malpractice insurance crisis:
The bulk of the dollars the insurers pay out in malpractice cases is in the form of settlements, not verdicts. In 2002, the year insurance carriers in New Jersey lost only 54 cases, they settled 732. Jury awards, Leone explains, put floors under the amounts for which suits can be settled. If juries have tended to award plaintiffs $1 million for a certain injury, the insurer knows it can't expect to settle a similar case for much less.
And the direction of verdicts and settlements, Leone claims, is up. In 1998, he says, Princeton's average payment to plaintiffs in malpractice cases against doctors was $235,000; in 2002 it was $343,000. The company's total payout to physician malpractice plaintiffs rose from $88 million in 1998 to $115 million in 2002.
Not to mention the money they spend reaching those settlements.
Speaking of Settlements: A while ago, when I posted a rant about lawyers seeking out injured clients, I got a barrage of email from lawyers who said this was not a common practice and that any lawyer who solicited clients would be disbarment material. Well, take a look at this story about people who make their living chasing down accident victims for lawyers:
Big business. Ask attorney David Shurtz. Each year, he pays out at least $100,000 to runners for referrals.
"Most of these people do not have anything beyond a high school diploma, and I know at least one of my investigators made $30,000 in a month," says Shurtz. (That's 50 cases at $600 apiece -- an extraordinary hustle.) Some of the runners are former clients. One was Shurtz's receptionist, who wised up, he says, when she realized she could make better money in fewer hours.
"I'm not ashamed of it," Shurtz says. "It's ethical. And if my greatest sin is giving $100,000 back to guys with high school diplomas who are out there working hard bringing in cases, send me to the gallows."
.....Personal injury cases can be sold to a lawyer for $300 to $600, sometimes more if the victim broke some bones or died. Not bad money. (They deal mostly in soft-tissue injury cases, which often get settled out of court, with the client netting a few thousand dollars.) Some runners say they can make $50,000-plus a year. Johnson estimates a runner can make up to $100,000.
...Some runners also offer money to potential clients to get cases.
"If I can get all of you signed up today, I'm offering all of you $150 apiece, that's cash money in your pocket," says one of the Fuddruckers lunchers while making phone calls in her car. She's just come out of the 5th District station with a notebook of names and numbers, including this bonanza: a vehicle that had three people in it when it was hit. That's enough business to justify $450 from her pocket.
"Solicit" must have a different meaning in legalese than it does in English.
SARS Epidemiology: The Lancet publishes the first study of SARS epidemiology today (online). The mortality rate appears to be quite a bit higher than the 4 to 8% we've been hearing:
The mean incubation period of the disease is estimated to be 6.4 days (95% CI 5.2-7.7). The mean time from onset of clinical symptoms to admission to hospital varied between 3 and 5 days, with longer times earlier in the epidemic. The estimated case fatality rate was 13.2% (9.8-16.8) for patients younger than 60 years and 43.3% (35.2-52.4) for patients aged 60 years or older assuming a parametric g distribution. A non-parametric method yielded estimates of 6.8% (4.0-9.6) and 55.0% (45.3-64.7), respectively.
Yet, no one in the United States has died from the disease, and worldwide the mortality is much lower. (See the New England Journal of Medicine'sgraph.) I suspect that the key to survival is to get early treatment. Even though there's no known drug treatment, early supportive care, such as ventilators and oxygen, probably make the difference. posted by Sydney on
5/07/2003 07:20:00 AM
0 comments
Tuesday, May 06, 2003
Alt Med Update: The wonderful world of herbal supplements has taken a hit in Australia. One company has had to recall hundreds of its products over safety and quality concerns:
More than 200 products were recalled in Australia this week when an audit revealed the company's breach of safety standards.
The problem widened last night when Australia's drugs watchdog added a further 449 products to the recall list.
That makes 668 products with possible health risks - and the Therapeutic Goods Administration indicated the list could reach 1000.
Pan is accused of substituting ingredients, manipulating test results and having substandard manufacturing processes.
Proving once again that herbal supplements are just as risky as any other drug, here's a description of one of the adverse reactions from taking the company's travel-sickness supplement:
The decision to withdraw all the company's products was made after 19 people were hospitalised after taking the travel medication Travacalm and dozens of others reported adverse reactions, including hallucinations that led to users attempting to jump out of the planes they were in. posted by Sydney on
5/06/2003 08:32:00 AM
0 comments
Friendship Means Sharing: Had to chuckle at the footnote to this SARS story:
A 60-year-old Gainesville woman, whom authorities declined to name, returned to Gainesville in late March after a visit to Beijing. She had a cough, but did not seek medical treatment until after she had coughed near a co-worker, a 47-year-old woman, whom she infected.
Both women were hospitalized in early April but have since fully recovered, according to Thomas Belcuore, health director for Alachua County. Neither showed signs of pneumonia and both are therefore still classified as suspect, rather than probable, SARS cases. They remain friends, Belcuore said.
Lessons: Ontario is taking the lessons learned by SARS to heart:
Ontario will launch a major overhaul of its hospital operations in the wake of the SARS outbreak, forcing changes in everything from basic infection control to the use of casual nursing help, Tony Clement, the Health Minister, said.
"We want to make sure that as a result of what I call the 'new normal,' our hospital system continues to be of the highest quality," Mr. Clement said in an interview. "Some aspects of hospital operations have changed forever."
The changes include less use of part-time nurses who work in several hospitals at a time, less transfer of patients between hospitals, and the recognition that hospitals need a "surge capacity" to handle unexpected epidemics. That's something hospitals here in the U.S. would do well to recognize, too.
And, as familiarity with SARS grows, so does our understanding of its natural history. Looks like it’s one of those viruses that can survive outside the body:
New laboratory findings support the theory that the SARS virus can survive up to four days on contaminated household surfaces like toilets but that disinfectants like bleach are effective weapons to kill it, the World Health Organization said yesterday.
The findings are important because doctors have determined that people infected with the virus can excrete it in large amounts in their stool and urine, raising the distinct possibility that less than vigorous hygiene - particularly a lack of hand-washing - can lead to its spread on surfaces in the home and elsewhere.
Health officials had assumed that this must be the case because of the pattern of spread in an apartment complex and hotel in Hong Kong. The new findings strengthen the theory, said Dr. Klaus Stohr, a German virologist and epidemiologist who is the scientific director of the W.H.O.'s SARS investigation.
Researchers at The University of Hong Kong found that disinfectants like bleach, ethanol, phenol, formaldehyde and paraformaldehyde can kill the virus, the W.H.O. said.
The findings should give further confidence that such measures, particularly in hospitals and homes where people who had contact with SARS patients are quarantined, will work, Dr. Stohr said in an interview.
The rest of the article has all the details on the viruses survival at various temperatures as well as its survival in various qualities of stool. (I don't envy the people doing those studies.)
But, the LA Times points out that it’s still unclear how all of this translates into communicability:
Stohr cautioned that the full meaning of the findings will not become clear until researchers learn how much virus is necessary to trigger an infection. That the virus can persist for hours on, say, handrails in a bus station may not be important if there is not enough of the virus present to produce disease....
.....Scientists remain convinced that the main way the disease is spread is through the coughs of patients. The greatest danger is thus to people in their immediate vicinity.
Not so Obvious: A reader recently emailed wondering about appendicitis, and how hard it is to diagnose. A couple of his friends had recently suffered the consequences of a delay in diagnosis - commonly referred to as a “ruptured appendix.” (It doesn’t really burst like a balloon. It’s just that the infection spreads beyond the appendix to the surrounding organs and abdominal cavity, a much more severe condition known as peritonitis.)
As it turns out, appendicitis isn’t always as straight forward as it would seem. A textbook case begins as pain around the belly button and progresses to a more localized pain in the right lower abdomen, accompanied by a lack of appetite. Often, there’s also vomiting, constipation, and fever. However, our bodies don’t read the textbooks.
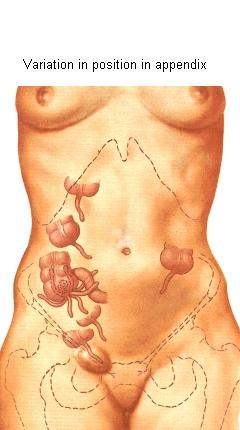
The appendix, a worm-like appendage of dubious usefulness, usually hangs straight down from the first portion of the large intestine, the cecum. However, like so many other things biological, the position of the appendix, and of the cecum within the abdominal cavity can vary widely. When an appendix sitting in a “normal” position gets infected and inflamed, it causes the classic textbook symptoms of right lower abdominal pain and tenderness. This, however, only happens about fifty percent of the time. An appendix sitting behind the obturator muscle causes a pain sensation in the pelvis, sometimes only detected with a rectal exam. An appendix behind the psoas muscle causes side pain. Sometimes, it hides behind the cecum, causing only mild pain in response to the doctor’s probing hands on the abdomen. In pregnant women, it gets even harder since the appendix can be displaced just about anywhere and shielded from examination by the enlarged uterus.
And, to complicate matters, most abdominal pain does not turn out to be appendicitis. Ovarian cysts, urinary tract infections, gastrointestinal viruses, and kidney stones, to name just a few, can present in a similar manner. And, since surgery is a risky business, doctors only like to operate if the likelihood of appendicitis is fairly high.
So, we're constantly searching for something that will increase our diagnostic certainty. Looking for higher numbers of white blood cells in the blood than usual is helpful, but not a certain indicator of appendicitis. Ultrasound can sometimes help to identify an enlarged and inflamed appendix, but it can miss cases, too. The state of the art at the moment is to use helical CT scans when in doubt. They give a high-resolution picture of the appendix that can pick up inflammation in surrounding tissue even at early stages. And, most importantly, they can identify a normal appendix.
If diagnosed within the first twenty-four to thirty-six hours, the surgical cure is relatively straightforward and simple. These days, it can be done laparoscopically, which means fewer surgical complications and a faster recovery time. Usually, patients go home the day after surgery if all goes well, leaving their appendices behind them.
Great Names: A physician in Britain named Marcus Aurelius recently passed away. Marcus Aurelius was the Roman emperor who financed Galen, the father of modern medicine. posted by Sydney on
5/05/2003 08:32:00 AM
0 comments
SARS Update: This week’s Lancet (free registration required) is full of SARS news. Turns out the disease is less severe in young children for some reason.
It also turns out that respiratory droplet precautions (masks, gloves, handwashing) are essential in preventing the spread of the disease:
All participants were surveyed about use of mask, gloves, gowns, and hand-washing, as recommended under droplets and contact precautions when caring for index patients with SARS. 69 staff who reported use of all four measures were not infected, whereas all infected staff had omitted at least one measure.
Maybe Chuck Simmins is right, after all. Sloppy precautions on the part of hospital staff members may have played a critical role in the disease’s spread. posted by Sydney on
5/05/2003 08:24:00 AM
0 comments
What's in a Name? William Safire has dug up the origin of SARS:
Here is how SARS the acronym came about. Three worried officials of the World Health Organization in Geneva, Switzerland, needed a name for a virus causing sudden deaths in China. The three were Denis Aitken, deputy director general; David Heymann, director of the Communicable Diseases Section; and Richard Thompson, its communications officer. (Presumably, he answers the phone with ''Communicable communications here.'')
''We wanted a name that would not stigmatize a location,'' Thompson says, ''such as 'the Hanoi Disease.' We first thought of A.P.W.D., or Atypical Pneumonia Without Diagnosis, and I'm glad we dropped that. Then we simply described the disease in another way, and it was in front of us -- Severe Acute Respiratory Syndrome, SARS.''
But what did they see as the difference between severe and acute?
''I asked this question, too, when we came up with the name. In medicine, severe is 'grave' and acute means 'suddenly.' This respiratory syndrome caused great harm (severe) and had a rapid onset (acute). Later, when we had conclusive evidence that a new coronavirus is the cause of the disease, we named it the SARS virus.'' posted by Sydney on
5/05/2003 08:15:00 AM
0 comments
Office Manners: I missed the essay in the Cleveland Plain Dealer that led to these letters to the editor, but evidently it was about encounters with doctors of the brief kind. This one struck a chord:
For a couple of years, I have noticed a new rival during office visits: The computer.
About 90 percent of my visit time is spent watching the doctor type into a desktop computer. The doctor sits facing the terminal, not looking at the patient, and type-type-types, with a few seconds of time-out every once in a while to ask me a question. Before I finish answering, the doctor has turned back to the terminal and types some more.
It's like having another person in the room who is getting all the attention, and I hate it! I feel like saying, "Excuse me, are you here today?"
If only that were unique to computers. I sometimes find myself doing the same thing with pen and paper. Unlesss it’s a straightforward encounter, I have to write down what the patient is telling me, or I’ll forget. Sometimes there’s just too much information coming at once to trust my brain; sometimes it’s things that are out of the ordinary. It’s so easy to get side-tracked, you wouldn’t believe. And memory is such a tricky thing - for patients and doctors. It’s much better sometimes to sacrifice politeness for accuracy. posted by Sydney on
5/05/2003 08:12:00 AM
0 comments
Public Health Militancy: Last week the New York Times ran an interesting graphic on its editorial page that showed the relative incidence of deaths from various diseases around the world. SARS occupied a tiny portion when compared to diseases like tuberculosis. (Unfortunately they didn’t make it available on the internet. Probably took up too much bandwith.) It illicited this response from one reader:
Howard Markel and Stephen Doyle present the real problem. The diseases enumerated demonstrate that our focus should be on public health, saving countless more lives than all the regime changes in the world.
Ah, but here’s the rub. Those diseases, like tuberculosis and HIV, are killing people in large numbers in nations with chaotic governments. Nations where the leaders live well and the people live miserably. (see the post below re: life expectancy) Nations where leaders starve their people for political reasons. You can hardly expect those governments to embrace public health measures to cut infectious disease. Which means that if those diseases are to really be eliminated, it would take a regime change. posted by Sydney on
5/05/2003 08:00:00 AM
0 comments
Apologies: No blogging today. The day was too beautiful to spend at the computer. Blogging resumes tomorrow. posted by Sydney on
5/04/2003 10:26:00 PM
0 comments
Saturday, May 03, 2003
Show Us the Money: One thing that's become clear in the past two years is that whenever America's public health departments are asked to do something, such as make contingency plans for potential bioterror attacks, they complain about it. There are only a handful of SARS cases in the United States, and here they are complaining about how much the disease is taxing them:
Seattle has yet to face its first confirmed case of severe acute respiratory syndrome, the stealthy, fast-moving illness that has caused panic and death from China to Canada.
But for Dr. Alonzo Plough, head of the Seattle-King County Public Health Department and for many of his colleagues around the country, the impact of SARS has arrived in full force, striking their agencies like a freak natural disaster.
"Very critical public health activities are not being done because of these very pressing demands of the moment," Plough said.
.....Plough calculates that SARS investigations and related work cost the department $160,000 in the first three weeks alone.
Goodness. How do they spend that money so fast? They say it’s spent tracking down contacts of possible cases, printing up multilingual patient-education signs for their public health clinics, and answering as many as six(!) phone calls an hour.
They claim to have had to investigate 60 possible cases of SARS in Seattle, but the CDC figures say that there have only been 44 in all of Washington. And six phone calls an hour? Staff at an average doctor’s office would think that a cakewalk.
But perhaps the most ridiculous of the arguments is this:
Dr. Laurene Mascola of the Los Angeles County Department of Health Services put the squeeze in blunt terms. "We have dealt with SARS to the detriment of other diseases," she said, pointing out that in California about 2,000 people die every month from unexplained pneumonia.
That figure seems high for just one state, especially since the entire nation, the death rate from pneumonia is around 64,000 annually. But, even if 2,000 people a month die of pneumonia in California, most of those deaths occur in people are at the ends of their lives (it isn’t called the “old man’s friend” for nothing). And the institutions that care for those people are hospitals and hospices, not public health departments.
But, of course, exaggeration is a critical tool when angling for more money. posted by Sydney on
5/03/2003 09:07:00 AM
0 comments
Trauma: Sally Satel notes that an army of psychologists may be about to be unleashed on the Iraqis, but will they really be needed?
A half-century of disaster research yields a largely sanguine picture of human response in the face of uncertainty, calamity and fear. The Center for Disaster Research at the University of Delaware has conducted hundreds of studies of natural disasters, chemical emergencies and building collapses. Over and over, researchers have found that people rarely panic or lapse into passivity.
Lee Clarke, a Rutgers University sociologist, has observed: "The rules of behavior in extreme situations are not much different from rules of ordinary life. . . . The most consistent pattern in disasters is that people connect in the aftermath and work to rebuild their physical and cultural environments." Most people are resilient and adapt well. They prefer to cope--and can cope--on their own. But the very idea that a potent stress could pose an ennobling challenge to the human spirit is the minority view among trauma professionals. posted by Sydney on
5/03/2003 08:33:00 AM
0 comments
PSA Screening:Dr. Jacob has an excellent post on the subtleties of prostate cancer screening. He's right, it's extremely difficult to discuss controversial screening tests like this without introducing your own bias. posted by Sydney on
5/02/2003 08:25:00 AM
0 comments
SARS Developments: Still trying to elucidate the natural history of the disease:
Researchers in Hong Kong reported that they had detected evidence of the virus in some people who have not gotten sick and in some who were thought to have recovered and, therefore, were no longer infectious.
"Some studies show people do continue to secrete the virus in feces and tears," said David L. Heymann of the World Health Organization, who was attending a scientific meeting on severe acute respiratory syndrome in Toronto. "Some cases actually recover and relapse. There are many more issues to be clarified."
But there have been no documented chains of transmission from SARS patients who have been released from hospitals, which indicates they may not be spreading the disease.
"We have to look at this," said Julie L. Gerberding, director of the Centers for Disease Control and Prevention in Atlanta. "The focus still needs to be on the people who are sick."
It isn’t uncommon for a virus to continue to be excreted in body fluids long after the illness is over. The virus that causes infectious mononucleosis is excreted for months, sometimes years, in body fluids, but only appears to be contagious during the early phase of the illness.
Guangzhou authorities divided the floor of People's Hospital No. 8 in half, putting SARS patients on one side of the elevator bank and AIDS patients on the other. Health care workers walked back and forth between the two sides, and some of those doctors and nurses contracted SARS.
Yet not one of the several dozen AIDS patients or their visitors, some of whom were also HIV positive, developed the disease. "I am wondering why there was no SARS virus co-infection in the AIDS cases," Dr. Zhang Fujie, director of AIDS treatment and care for China, said yesterday in an interview. "We are exchanging information with Hong Kong on this. We will continue to try to understand that."
Dr. Cheng Feng of the China/UK HIV/AIDS Project said he, too, was aware of the phenomenon. He wondered whether the drugs the AIDS patients were receiving for HIV control might be blocking a SARS infection. A similar notion was mentioned by Dr. Yuen Kowk-yung of the University of Hong Kong. With New York's Dr. David Ho, of the Aaron Diamond AIDS Research Laboratory, Yuen is exploring the AIDS apothecary for an effective SARS treatment.
It could be the drugs, or as Andrew Sullivan points out, it could be that the immune system’s response to the virus is the primary cause of the illness. That would help explain why so many of the victims are young and healthy, and why steroids, which suppress the immune system seem to help. posted by Sydney on
5/02/2003 08:18:00 AM
0 comments
Class Action: Efforts at tort reform are still quietly proceeding. According to this story about a bill in the Senate to reform class action lawsuits, some of those settlements are right out of a Seinfeld episode:
Class-action suits have also become an ATM for unscrupulous lawyers, who win millions of dollars for themselves but sometimes leave clients empty-handed. Last year, lawyers suing Blockbuster Video reached a settlement giving their clients coupons for free movie rentals. The lawyers pocketed $9.25 million - and Blockbuster was allowed to continue the late-fee practices that triggered the lawsuit. Plaintiffs suing Columbia House record club got nothing but a discount on future purchases. Their lawyers took home $5 million, plus expenses. Sometimes, plaintiffs lose money while lawyers get fat fees.
And, on the medical malpractice front, the Senate will soon be considering the issue, but whether or not they’ll get to vote will depend on the behavior of the Democrats:
The Senate will soon consider a medical liability reform bill, following last month's passage by the U.S. House of Representatives of the White House-sponsored Health Act, which would limit punitive damages in malpractice cases.
"We realize this is an uphill battle," Purdon said. "Some Democratic senators have threatened to filibuster
Dr Roy Kessels, from the University of Utrecht in the Netherlands found that between half and four-fifths all all medical information delivered during an average consultation was forgotten instantly by the patient.
In addition, half of the information that managed to gain a foothold in the memory of the patient was later recalled incorrectly.
The problem was particularly acute in older patients, he found, or in those who were anxious about bad news.
The elderly and the anxious are understandable, and there are some patients who need to have everything written down so they won't forget, but there are also a large number of people who just aren't capable of listening. You can see it in their eyes - they're thinking about the next thing to say as you explain your treatment plan, and they never let you finish a sentence. They say that doctors interrupt their patients frequently, (the implication being that we don't listen), but I'd like to see a study on how often patients interrupt their doctors. posted by Sydney on
5/01/2003 09:04:00 AM
0 comments
Misunderstanding: A reader sent along this Reuters account of a study published last month in JAMA:
The average weight loss among Weight Watchers participants "is not very much in comparison to what people hope they will lose, or what people need to lose in order to reach the desired, svelte self," study author Dr. Stanley Heshka told Reuters Health.
These findings suggest that people who need to lose a significant amount of weight fairly quickly for medical reasons may want to opt out of Weight Watchers and similarly structured programs, said Heshka, who is based at the New York Obesity Research Center, St. Luke's/Roosevelt Hospital in New York City. In the program, participants attend weekly meetings and receive guidelines for exercise and how to pick the healthy foods and portions.
To be fair, the article goes on to point out that Weight Watchers is just as successful as any other weight loss program, and in fact superior to doing it on your own, but the overall impression one gets from it is that Weight Watchers doesn’t work. The study in fact found that people on Weight Watchers lost more weight:
At 2 years, 150 participants (71%) in the commercial group and 159 (75%) in the self-help group completed the study. In the intent-to-treat analysis, mean (SD) weight loss of participants in the commercial group was greater than in the self-help group at 1 year (-4.3 [6.1] kg vs -1.3 [6.1] kg, respectively; P<.001) and at 2 years (-2.9 [6.5] kg vs -0.2 [6.5] kg, respectively; P<.001). Waist circumference (P = .003) and body mass index (P<.001) decreased more in the commercial group. Changes in blood pressure, lipids, glucose, and insulin levels were related to changes in weight in both groups, but between-group differences in biological parameters were mainly nonsignificant by year 2.
The structured commercial weight loss program provided modest weight loss but more than self-help over a 2-year period.
The truth is that losing weight and keeping it off is extremely difficult. It requires a degree of obsession to detail (counting calories) that’s difficult to sustain. Quitting tobacco or alcohol is easy in comparison. It isn’t that difficult to avoid cigarettes or spirits, although you might have to give up social outlets to do so. It’s impossible to avoid food completely, so the temptation to overeat is always there. That’s not to say that it can’t be done; just that it is, in some ways, a Herculean task. posted by Sydney on
5/01/2003 08:47:00 AM
0 comments
SARS Shenanigans?Chuck Simmins says he's suspicious about the WHO's reasons for lifting the Toronto travel ban:
More good Canadian info. Illustrating the perils of recordkeeping, I suppose. WHO lifts its ban on Toronto because no new cases have been reported in 20 days, and the very same WHO reports four new cases in Canada during the period 4/28 to 4/29. The Canadian gov't site reports two more probable and eight more suspect in the same time frame, the two probable and four of the suspect are in Ontario.
I think it's fair to say the WHO really didn't lift its ban because there hadn't been any new cases... Just that they got so much flack about it.
When Toronto began fussing about the travel ban last week, one WHO official was quoted by the Times as believing any lifting of it would be due to political, not medical, realities. Chuck's data seems to support this:
The WHO accounting of Canadian cases as of April 30.
The figures speak for themselves.
And speaking of honesty as policy, Dissecting Leftism is attempting a one-man battle to bring transparency to that bastion of dishonesty, China:
The Chinese seem to have become really serious about internet censorship in recent months. They re-blocked Blogspot some time ago and lots of other sites are blocked too -- including at least some Lycos and some Yahoo. I have therefore decided to do my tiny bit towards keeping communications open by putting a mirror of my blog up on a site that China does NOT block. I keep all my blog entries as a file so once I have written my blog entries for the day, it takes me only a couple of minutes extra to put them up on a second site. So in future my blog will also be accessible at the following address: http://members.optusnet.com.au/~jonjayray/tripod.html. The site concerned is hosted by my local ISP so it may stay too insignificant to be blocked by China. With ISP hosting, the site is also advertising-free, which is a bit of a bonus. I will also be putting up my "China" postings several hours before I put them on Blogspot. Because Blogspot is so trouble-prone, I do not post there until just after midnight, California time, in the hope that the load and the errors will be minimal then. I would be much obliged if anyone with contacts in China would let them know of the new site. I even have some archives there so people can catch up with what was posted in the last 6 weeks or so. posted by Sydney on
5/01/2003 08:25:00 AM
0 comments
Nukes, Bugs & Poison:Winds of Change has a collection of news and reflections on all security threats biological, chemical, and nuclear. posted by Sydney on
5/01/2003 07:50:00 AM
0 comments
Weekly Art History Lesson: Claude Monet (1840-1926) saw the world as a fantastic mixture of color and light. How much of that world view was due to genius and how much to faulty eyesight, we’ll never know, but legend has it that when once fitted with eye-glasses to correct astigmatism, he threw them away, saying, “If the world really looks like that I will paint no more!”
What better subject for an artist of color and light than a field of tulips?
Tulip Fields in Holland,1886
Painted in the late 1880’s, when success finally left him well-off enough for a series of travels, the painting is a landscape unique to Holland - the quintessential Dutch windmill surrounded by a sea of tulips. It is a blurred panorama of light and color that leaves one wishing the focus could be adjusted ever so slightly.
How a flower from the high, rocky mountains of Pakistan ever came to be the agricultural mainstay of a marshy, low-lying northern European country is a story in itself. It is, in many ways, the story of beauty made possible by science and technology. It was the engineering feat of the windmill which made the marshy fields dry enough for successful bulb cultivation by pumping the excess water into canals that drain to the sea. And it was the science of pharmacology that brought the flower to the marshes.
It was a French pharmacologist, (back when pharmacologists were botanists, not chemists), who introduced the tulip to Holland. Charles De L'ecluse (aka Carolus Clusius), was forced to flee in succession not only his native France, but academic posts in Prague and Vienna because of his Protestant beliefs. He accepted the post of head botanist at the University of Leiden in 1593 with the intent of establishing a medicinal garden such as those in Vienna and Prague which had established his reputation. Among his collection of plants was the tulip, given to him by the Viennese ambassador to the Turkish court of Suleiman the Magnificent.
The tulip became one of the most popular flowers in the Leiden garden, although it had no medicinal value. Clusius was loathe to share his specimens, but contraband bulbs lifted surreptitiously from his garden made their way to private hands. Eventually, with time and hybridization, they gave birth to the brightly colored fields of modern Holland - and the Holland of Monet.
Monet, on seeing those fields, described them as “enough to drive a poor painter crazy - impossible to render with our poor colors,” but render them he did in his astigmatic but beautiful way.
Unfortunately for Monet, his vision continued to fail as he got older. Astigmatism gave way to cataracts, which not only robbed him of clarity, but of color perception. By the end of his life, he was quite blind; his view of the world unquestionably altered, but no less beautiful. posted by Sydney on
5/01/2003 07:24:00 AM
0 comments





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}