"When many cures are offered for a disease, it means the disease is not curable" -Anton Chekhov
''Once you tell people there's a cure for something, the more likely they are to pressure doctors to prescribe it.'' -Robert Ehrlich, drug advertising executive.
"Opinions are like sphincters, everyone has one." - Chris Rangel
Mother Theresa's Miracle: There was some controversy over the miracle that supported the beatification of Mother Theresa:
The sole miracle that was approved by the Vatican and pushed her towards beatification involved Monica Besra, a tribal woman from Balurghat in North Bengal, who claimed to have been healed of a reportedly incurable abdominal tumour after she prayed to Mother.
Following the claim, the then Archbishop of Kolkata Henry D'Souza constituted a five-member tribunal within the Diocesan Inquiry Team, including doctors and scientists and priests, to examine its veracity.
While the tribunal recorded Besra's case as a "genuine miracle", doctors who treated her at the Balurghat and Raigunj hospitals challened her claim, saying that she was cured as a result of medical intervention.
As the controversy raged on, a section of the clergy demanded that Besra's claim be re-examined and, if necessary, rejected to uphold the objectivity and credibility of Church inquiries.
Unmoved by the controversy, the Vatican asserted that the miracle was a "fait accompli" and that it had no intention of re-examining the case.
It's hard to be a saint in the modern world. Lucky for those who would be saints, the Vatican doesn't live in the modern world. posted by Sydney on
12/21/2002 09:27:00 AM
0 comments
Manna: Pat Robertson not only pitches God to millions, he pitches health food, too:
Condemning the evils of ``syrup-drenched hot cakes,'' television evangelist Pat Robertson is pitching his own ``Age-Defying Protein Pancake'' to the millions who watch him daily on The 700 Club.
Robertson, 72, cooked up a stack of the pancakes during a broadcast last month on the Christian Broadcasting Network, which Robertson founded and heads.
Within 48 hours, 38,000 people had called for the recipe or had downloaded the preacher's pancake off the CBN.com Web site.
The high-protein flapjacks are credited by Robertson with helping to protect against breast, uterine and prostate cancer, and with fighting the buildup of plaque in blood vessels.
``My mother taught me to cook when I was a little boy, and I've been relatively good at it,'' he said.
The griddle cake is the third nutritional promotion by Robertson, who also extols ``Pat's Age-Defying Shake'' and ``Pat's Age-Defying Antioxidants.''
None of the promotions sells a product. Instead, Robertson provides recipes with ingredients, such as soy flour and plain yogurt, and identifies specific vitamins and minerals that help protect against disease. posted by Sydney on
12/21/2002 09:22:00 AM
0 comments
Gift of Health:USA Today has a list of medical gifts. Among such items as therapeutic massage, yoga videos, and music therapy CD’s are some of dubious merit. Some, in fact that might end up costing your loved one more money with no added benefit:
Ultra-fast CT scans: The CT scans are advertised as a means to find tumors and heart disease that you might not be aware of. The problem is, they have more of a tendency to find uncertainties than disease. Cardiac CT’s measure the calcium content in the coronary arteries, but we don’t know how much calcium indicates a problem, and calcium is found in the arteries of most people over the age of 25. The finding of calcium usually leads to more testing - often a cardiac catheterization. Cardiac catheterizations are both invasive and expensive, and not to be undergone lightly.
CT scans to screen for lung cancer are of dubious worth. Ditto abdominal scans. Both may lead to unnecessary biopsies, which in the case of the chest and abdominal cavities involve invasive, expensive, and risky procedures.
PSA: This is the blood test that can detect early prostate cancer. It isn’t very good as screening tests go. The PSA can be increased when the prostate is benignly enlarged, or when it has cancer. Furthermore, many prostate cancers are very slow growers. Men can live with them for years and end up dying of something else. Having a postive PSA can lead to prostate biopsy. If cancer is confirmed, there’s then the very difficult decision of what to do about it - complete removal of the prostate, with its attendant complications of impotence and incontinence, or watchful waiting and observation?
Female Hormone Panels: These are blood tests that can tell whether a woman is in menopause or not. Little harm is likely to come from doing them, but the question is why do them? Women who have all of their reproductive parts will know they’re in menopause when they stop having periods. Women with hysterectomies may have trouble knowing when menopause is upon them, unless they have symptoms such as hot flashes or vaginal dryness. But, in the absence of symptoms, there’s little reason to intervene. Hormone replacement therapy has turned out to be devoid of the health benefits we used to claim for it, and is now only recommended for symptomatic treatment of menopause. Testing for hormone levels isn’t likely to provide any useful information that can’t be had by simply asking about symptoms. posted by Sydney on
12/21/2002 09:15:00 AM
0 comments
Vanity Scam: There's a company out there that claims to make personalized skin cream based on the customer's genetic code:
After answering a 10-minute online questionnaire about their skin -- about ethnic origins, pore size, climate, hydration -- customers get the inside of their mouths swabbed for a DNA sample. The test and the sample are sent to a lab to be analyzed, with customized skin creams generated based on the results. The tub of cream even has your name on it.
But the personal treatment comes with a hefty price tag: $250 for a 1.7 ounce jar of the DNA cream.
There's probably some validity in making skin cream based on climate and skin characteristics, but the DNA information would provide absolutely no useful information. And $250? If that were a prescription skin cream, there would be cries of outrage. Funny that, we're willing to pay more for unproven therapies than we are for proven therapies. posted by Sydney on
12/21/2002 08:26:00 AM
0 comments
Friday, December 20, 2002
More Smallpox Vaccine News: Germany is increasing their stockpile of vaccine, and in Ohio, healthcare workers who have side effects from voluntarily taken vaccines will be covered by worker's compensation benefits:
"Already volunteers, these health care professionals are performing a valuable service protecting their communities. They need to know we will be there to protect them," said James Conrad, the bureau's administrator and chief executive.
Monopoly: South Knox Bubba says that insurance companies are like the Mafia - deal with them on their terms or else. (Gee, and I thought only doctors felt that way.) posted by Sydney on
12/20/2002 01:02:00 PM
0 comments
Smallpox Vaccine Issue: The public debate about smallpox vaccine has a forum in the pages of the New England Journal of Medicine, or at least at their website, where they’ve provided full access to articles that will be published in January. They include the statistical methods that were used to calculate the risk of spread of the disease in the event of a bioterror attack (rather conservative in their estimates of its contagiousness), and the anecdotal approach based on the author’s experience in Pakistan in the 1970’s. The latter, by the way, is wildly optimistic when it comes to the disease, but extremely pessimistic when it comes to the vaccine. Even in the face of an attack.
There’s also a review of past cases of transmission of cowpox from the vaccinated to the unvaccinated. Bear in mind that hygiene and universal precautions weren’t nearly up to modern standards back then, as this case of urinary-catheter transmitted cowpox demonstrates :
After her older brother received vaccine,a 13-month-old girl had initially undiagnosed genital lesions and dysuria resulting from vaccinia infection.At the hospital,she was catheterized,and the catheter was then placed in a pan of Citrosil solution for sterilization.Several other urinary catheters were soaking in the same pan.Within a five-week period,there were 23 secondary cases with vulvar urethral vaccinia;each of the patients had been catheterized with one of the contaminated catheters. About half had high fevers,and some had gross hematuria.Virus was cultured from the urine of several children.
It’s also quite possible that many of the hospital-transmitted cowpox cases were transmitted through the bed linens, which would have been changed daily and laundered together. It might be prudent to recommend that those who receive the vaccine launder their clothing separately, and of course to keep their vaccine site covered with a bandage at all times.
There was also this:
“...many hospitals remain uncomforable with the recent recommendation against the provision of administrative leave for newly vaccinated health care workers.”
Who made that recommendation? If hospitals are concerned that vaccinated workers would transfer cowpox virus to their patients, then they should insist that their vaccinated workers stay home until their vaccine site heals. It wouldn’t take all that long, a matter of days. And introducing a voluntary vaccine program now, when coverage of absences can be planned and arranged, makes more sense than waiting for a smallpox attack, when vaccination has to be quick and universal, especially among exposed healthcare workers, and when they would be needed on the job even more.
The best piece in the Journal’s collection, though is the public survey about smallpox and smallpox vaccine. People support the current policy of voluntary vaccination, but they’re suspicious of what would happen if the vaccine had to be offered quickly to massive numbers of people:
The respondents were asked about two of the policy issues currently being debated: vaccination of health professionals and vaccination of the general public.A strong majority (81 percent)of the repondents favored voluntary vaccination of doctors United States (Table 2). Moreover,72 percent believed that if it was not possible to vaccinate everyone quickly,wealthy and influential people would get the vaccine first;43 percent believed that the distribution of the vaccine would discriminate against the elderly,and 22 percent believed that it would discriminate against blacks. (emphasis mine)
Voluntary vaccination of healthcare workers also seems the wise thing to do when you consider that people say they would go to their own doctors and to emergency rooms if they thought they had smallpox:
Approximately half the respondents (52 percent) said they would go to their own physician first for diagnosis and care if they thought they had smallpox, 40 percent would go to a hospital emergency room, and 7 percent would go to their local health department (Table 3).Most of the respondents were confident that their own physician would recognize the symptoms of smallpox (43 percent were very confident,and 40 percent were somewhat confident).
In fact, one of the other pieces on the Journal’s website was a paper describing just what happened when a man in Cleveland presented with a disease similar in appearance and symptoms to smallpox. His doctors had to scramble to send specimens to the CDC in Atlanta for special testing. There was no place in Ohio capable of doing the tests. They had to fill out special forms, by typewriter, to get a courier to handle the specimen and deliver it to Atlanta, and they faced a time deadline to get it to the courier’s office. What they don’t mention in this paper, but which was detailed in a Cleveland Plain Dealer article about the same case last month (no longer on line), is that before the man turned up in these doctors’ offices, he had also been to two emergency rooms and a family practice clinic. No one in any of those places considered smallpox. If it had been smallpox, a good many people would have been exposed by the time it was recognized. It underscores the dire need for physician education on bioterror, and the importance of voluntary vaccination among healthcare workers.
But back to the survey. It also asked about people’s attitudes toward the vaccine. They apparently harbor no illusions about its dangers:
Although serious adverse reactions to the vaccine are expected to be relatively rare in patients without contraindications to the vaccine, a substantial proportion of the respondents thought that serious complications from the vaccine,including death,would be likely.
So much for the argument that the public has unrealistic expectations of the vaccine’s safety. posted by Sydney on
12/20/2002 08:27:00 AM
0 comments
Smallpox Vaccine Defense: The American Academy of Family Physicians have taken the middle road on the smallpox vaccine. They support voluntary vaccination of health care workers, and caution the public to take the time to learn about the vaccine before volunteering to have it. That’s a sensible approach, free of political hysteria.
Meanwhile, my local health department finally sent out physician education material about smallpox, including a 24-hour phone number to call in case of a threatened case. It also included a list of internet learning resources. Unfortunately, this still leaves a significant number of phyisicans who don’t use the internet out of the loop. They did say, however, that they’re working on some educational programs for bioterror defense. I’m guessing that the announcement of the Administration’s smallpox vaccination plans has lit a fire under them and made them take the threat of bioterrorism seriously. posted by Sydney on
12/20/2002 07:58:00 AM
0 comments
Genetic Revolution Update: Researchers have used genetic profiling to predict the invasiveness of breast tumors:
But scientists said the genetic signature — the activity of a collection of 70 genes — appears to predict cancer mortality better than traditional measures like tumor size or stage or whether the cancer has spread to a woman's underarm lymph nodes.
In the study, 5.5 percent of women whose cancers had a good genetic signature died within the next decade, as against 45 percent of those with bad genetic signatures.
That’s pretty impressive, and much better than any of our other methods of predicting the potential for a breast tumor to spread. The main page of the New England Journal of Medicine’s website has a photo of the the microarray used to profile the tumors. And the Times article in the above link has a nice graphic explaining the process, although it isn’t linkable. (The link is to the right of the article’s text.) posted by Sydney on
12/20/2002 07:40:00 AM
0 comments
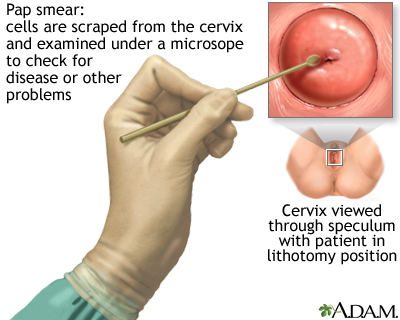
Among those who do not need Pap tests, the cancer society says, are women who have never had sexual intercourse, women who have had total hysterectomies that included removal of the cervix for reasons other than cancer and women age 70 or older who have had three or more normal Pap test results and no abnormal results in the last 10 years.
Few tears will be shed over this, unless they're tears of joy. Most women would rather have a root canal than have a pap, but the new guidelines don't mean that the yearly pelvic exam is a thing of the past. In fact, the guidelines only refer to the pap test itself, the act of swabbing up random cells from the cervix and sending them off to the lab. Women should still have pelvic exams to check the vaginal walls for tumors, and warts; to check for uterine enlargement or ovarian tumors, and to check for sexually transmitted diseases. So, check those cheers and buck yourself up to continue on with the dreaded yearly pelvic. posted by Sydney on
12/20/2002 07:39:00 AM
0 comments
Battle of the Clones: Now a Canadian cult says that it can beat the Italian gynecologist in the race for a human clone. The group says that its baby will be born around Christmas. posted by Sydney on
12/20/2002 07:38:00 AM
0 comments
Thursday, December 19, 2002
Spot On:The Washington Post editorial on the decision of two teaching hospitals not to offer the smallpox vaccine to their employees gets it exactly right:
Doctors who administer teaching hospitals, on the other hand, have a different sort of responsibility to the community. Their job is not to assess intelligence risks or to second-guess state public health officials but to be prepared to care for sick people, and to vaccinate healthy people, in case an outbreak should occur. Clearly, health care workers are also among those most likely to be infected, particularly in the early stages of an epidemic, because they might come into contact with sick people before the disease is identified. Without a core group of immune health workers, it will be hard to respond at all to a mass outbreak of the disease. At the least, hospital administrators owe it to their own personnel to make the vaccine available, and to explain the risks of receiving it or refusing it, before dismissing the validity of the vaccination campaign out of hand.
It is the height of arrogance to make the decision for their employees - the embodiment of paternalistic medicine. Nor does their claim that the President’s recommendations are “politically motivated” reflect well on them. It only makes their own position appear politically motivated. Let’s face it, academic medicine isn’t immune to the political leanings of the rest of academia, and in denying a voluntary vaccine to their employees, these academics are making sure that their institutions will give no aid to the war effort. Either that, or they’re just acting as selfish employers who want to avoid employee absence due to side effects of a vaccine. posted by Sydney on
12/19/2002 04:37:00 PM
0 comments
CORRECTION: I originally posted this correction on Dec. 16, at the bottom of the post called "Insurance Conundrum," but evidently many missed it. Both the University of South Dakota School of Medicine and I have gotten the acronym wrong for that irksome piece of legislation, correctly called HIPAA - Health Insurance Portability and Accountability Act. I can't speak for the South Dakota Medical School, but I know my error comes from seeing somanyimagesofhippos associated with it. posted by Sydney on
12/19/2002 03:46:00 PM
0 comments
Sometimes Cheaper is Better: Or at least just as good. Those of us who have stuck by the old, cheap, and effective water pills for high blood pressure have just been vindicated. Turns out that they're not only cheaper than newer drugs, they're just as effective. A large and comprehensive study compared thiazide diuretics, one of the oldest blood pressure medications around, with the newer ACE inhibitors (angiotensin converting enzyme inhibitors) and to calcium channel blockers:
Compared to participants who took the diuretic, the ACE inhibitor group had, on average, about two points higher systolic blood pressure, the top number in the blood pressure reading. Blacks in the group had a systolic blood pressure four points higher.
There was a 15 percent higher risk of stroke overall for the ACE inhibitor group and a 40 percent higher risk for blacks. The risk for heart failure among all groups was 19 percent higher, and the risk for hospitalization or treatment for the chest pains of angina was 11 percent higher. Further, the risk of needing a coronary bypass operation or angioplasty was 10 percent higher.
Compared with participants who took the diuretic, the calcium channel blocker group had, on average, a systolic blood pressure about one point higher and a 38 percent higher risk of developing heart failure
Although the press have been making diuretics out to be superior to the newer drugs, the truth is they’re really about the same. The mean blood pressure readings were the same for the diuretics and the newer drugs. (They differed by only two to four points, not a clinically significant difference at all). The incidence of heart attacks and other illnesses were basically the same, too, varying by only one or two percentage points.
This does, however, have quite a bit of significance for treatment. Many physicians have been led down the primrose path of believing that ACE inhibitors are the superior drug. Not, as the Times suggests, because we’ve been brainwashed, but because of theoretical advantages of ACE inhibitors in heart patients. These theories have been backed up by studies. It is true that those studies showed marginal improvement, and that their authors gave them the best possible spin they could, but they were published in prestigious medical journals. And when a study gets published in a prestigious journal, the theory gets transformed into gospel. (Which is a rant for another day) Now, we have data that calls that theory into question. In the real world, the newer drugs have no advantage over the old drugs, although they cost a much prettier penny. Lisinopril, the ACE inhibitor used in the study costs from $12 to $25 a month , while chlorthalidone, the diuretic used costs $8.
There are still some conditions, though, in which an ACE inhibitor would be a better choice. They slow the progression of kidney disease in diabetics, for example. And they can improve the function of a failing heart. But for the average, uncomplicated case of high blood pressure, there’s no good reason to avoid a trial of the cheaper drugs.
ADDENDUM: Derek Lowe has the medicinal chemist’s view here.
And Statins Aren’t So Great, Either: The same study that looked at diuretics also looked at the value of Pravachol, a cholesterol-lowering drug, which along with others in its class has been hailed by some as the miracle drug of the late twentieth century . The study compared mortality rates in people with high blood pressure and high cholesterol who were treated with diet versus those who were treated with the cholesterol-lowering drug.
The statins have earned their all-star status on the basis of studies that show they improve the incidence of heart attacks by a few percentage points. If you look at the rates of death, however, they don’t give any advantage:
Pravastatin did not reduce either all-cause mortality or CHD significantly when compared with usual care in older participants with well-controlled hypertension and moderately elevated LDL-C. The results may be due to the modest differential in total cholesterol (9.6%) and LDL-C (16.7%) between pravastatin and usual care compared with prior statin trials supporting cardiovascular disease prevention.
Apologists for statins say that the results are the same because many in the diet group ended up on statins during the study, and many on statins had to stop them. Why did some in the diet group end up on statins? Because giving statins to patients with other conditions such as heart disease or diabetes has become the standard of care in this country - despite the marginal benefits of doing so. And why did some of those taking the drugs stop? Side effects. However, if you look at the numbers, you can see that these subgroups were in the minority, and likely to have had little effect on the outcome.
And yet, there are those who just can’t, or won’t, give up on the statins as saviours point of view:
"Physicians might be tempted to conclude that this large study demonstrates that statins do not work," according to Dr. Richard C. Pasternak, of Harvard Medical School in Boston, Massachusetts. "However, it is well known that they do," he concludes in an editorial that accompanies the study.
What may have happened, according to Pasternak, is that the drugs may not be as effective in ordinary settings as they are in clinical trials where participants are carefully selected and followed closely.
Pasternak has served as a consultant to or on the advisory boards of several pharmaceutical companies, including Bristol-Myers Squibb. In addition, he has received funding from Merck-Medco and has served on the speakers bureau for several drug makers.
It isn’t well known that they work. What is well-known is that they provide a marginal benefit (Click here, here, here, and here for the studies, and here for my rant) at great financial costs - at least for patients and insurance companies, if not for Dr. Pasternack, and his colleagues. And most of us live and work in the real world, not in the rarefied atmosphere of a clinical study.
Marriage of Medicine and Physics: Doctors in Italy have treated metastatic liver tumors by removing the liver from the body and irradiating it in a reactor:
The organ was placed in a Teflon bag that neutrons can pass through and taken to a research reactor nearby, where it was irradiated with neutrons. It was then re-implanted, just as in a normal liver transplant operation.
"By explanting the organ, we could give a high and uniform dose to all the liver, which is impossible to obtain inside the body without serious risk to the patient," says Tazio Pinelli, a physicist who coordinated the work together with liver surgeon Aris Zonta.
It's only been tried on one patient, a man with colon cancer that had spread to his liver, but after one year, they say he's alive and well. posted by Sydney on
12/19/2002 07:16:00 AM
0 comments
Virgin Birth: Renegade Italian gynecologist and mad cloner Severino Antinori claims that the first human clone will be born next month - in Serbia. Oh, well. Bosnia has a virgin mother, why not Serbia? posted by Sydney on
12/19/2002 07:15:00 AM
0 comments
Rote Memorization: A paper in Nature Neruoscience says that good memorizers have ordinary brains:
"Superior memory was not driven by exceptional intellectual ability or structural brain differences.
"Rather, we found that superior memorisers used a spatial learning strategy, engaging brain regions such as the hippocampus which are critical for memory and for spatial memory in particular."
In other words, they use mnemonics, the favored memorization system of medical students everywhere. posted by Sydney on
12/19/2002 07:14:00 AM
0 comments
"The message for John Manley is: health-care dollars, health-care dollars, health-care dollars," Ecker declared after she and other ministers met in preparation for pre-budget talks with the federal finance minister.
"The needs are there today," Ecker told reporters. "I don't know how any political leader in this country can say to their citizens that we don't have health-care needs today."
What the political leaders are saying is that the money isn't there today. That's the problem with single-payer health care. The need always outstrips the means. And the need is always a handy tool for achieving political ends. posted by Sydney on
12/18/2002 10:16:00 AM
0 comments
Smallpox Past and Future: Yesterday's New York Times ran a first hand account by one of their editors of post-vaccine encephalitis. He's right about the need for a full and comprehensive effort at public education about the vaccine before it's offered to the public. Efforts should begin now, before it becomes available and not later. The Times is to be commended for the role it's played so far in reporting impartially on the vaccine's side effects and on the dangers of smallpox the disease.
Meanwhile, plans are being made by an American company to test a supposedly safer Japanese version of the vaccine. How much safer, and whether or not it's effective are unknowns:
Dr. Donald Francis, the president of VaxGen, conceded that the testing in Japan in the 1970's might not have been extensive enough to detect serious complications, which are rare even in the conventional vaccine.
Moreover, since the Japanese vaccine is a live virus, it is not likely to be recommended for people who should not take the existing vaccine, like those with compromised immune systems or certain skin disorders, VaxGen executives said.
Medical Errors:The New York Times editorial page weighs in today on the issue of medical errors. Forget for a moment their repetition of the lie that won’t die - the statisitcally flawed , overinflated estimate of deaths due to medical errors, and concentrate instead on their lamentation that physicians are a barrier to minimizing error:
Less than a quarter of the doctors think it would be very effective to use computers instead of paper forms to order drugs or to include pharmacists on hospital rounds, two approaches that have been shown to reduce medication errors in hospitals. Nor were they enthusiastic about using only specially trained physicians on intensive care wards, or about limiting high-risk medical procedures to hospitals that do a lot of them, despite evidence that expertise and frequent practice are key ingredients in successful medicine.
Errors, regardless of how low their incidence, should be minimized. It would be wonderful if we lived in a perfect world where errors could be completely eliminated, but we don’t. And since we live in the real world, we should consider the consequences carefully of any steps we take to reduce errors. They may introduce errors of their own.
Including pharmacists on hospital rounds, for example, may be an achievable goal in some situations - say in teaching hospitals where rounds are done by teams of residents and attendings at set hours of the day. But most hospitals aren’t teaching hospitals, and most rounds aren’t done by teams of physicians, but by the patient’s own attending physician. It would be impossible to coordinate the visits of every community physician to the hospital to see their handful of patients with the pharmacists’ schedule. I’d rather have the pharmacist in the pharmacy making sure drugs are mixed properly, or checking a database for potential drug interactions. Making the pharmacist abandon the pharmacy for rounds would be an extremely wasteful use of a pharmacist, even if you could coordinate his schedule with all of the rounding physicians at a hospital. Drugs aren’t ordered every day, or changed every day in most hospitalized patients. In most cases, rounds amount to monitoring the progress of a patient well on their way to healing.
The intensivist issue is a little trickier. In large hospitals, intensivists make sense. Because they serve a large population, they have more critically ill patients, and having one or two physicians in charge working as a team with the nursing staff is a more efficient use of resources, and translates into better care, especially if the patient's primary care physician is included. But, not all hospitals serve large communities. There are plenty of small community hospitals far from a large city, where people end up needing short-term critical care - say a ventilator for pneumonia or emphysema, or they need stabilization in a critical care unit for a devastating illness before they can be safely transferred to the distant, larger hospital with its specialty care. In these situations, an intensivist isn’t necessarily a requirement, or even that much of an enhancement. He may, in fact, languish in a small community because his skills aren’t in much demand. A general internist, family physician, pulmonologist, cardiologist, or hospitalist with intensive care skills and experience could just as easily handle this sort of situation, and be more likely to survive financially since they provide other sorts of care as well.
Then, there’s the issue of computers. Computers are wonderful. Their influence on our lives for the better can’t be denied. But they aren’t a panacea for every ailment. Errors are just as likely to occur when data is entered into a computer as when it’s written on an order form. It’s much harder to inadvertently handwrite a wrong number than it is to inadvertently enter it on a computer keyboard. The handwritten order has to be read and interpreted by another person, usually the nurse caring for the patient, who is more likely to notice an error than a computer system would. In the computer system, the order gets automatically translated into action by people who don’t know the patient at all.
Consider the hospital error that happened to a patient I saw this past weekend. She was a patient of a colleague, admitted for pneumonia. When I went to see her on Saturday morning, she wasn’t in her room. The unit clerk told me she was getting an echocardiogram. That struck me as odd, because my colleague hadn’t mentioned it to me, and she hadn't mentioned anything that would warrant an echocardiogram. Maybe she forgot. Later, when the patient had returned, and I could look through her chart, I discovered that there was no order for an echocardiogram. What had happened was that the clerk entering the order into the computer had typed an “8” instead of a “9” when she was entering the room number. The order went down to the cardiac lab, who sent someone up to get the patient from that room. Luckily, an echocardiogram is noninvasive and painless and without risk. The only damage from doing it on the wrong person is that she might have to battle an incorrect hospital charge. But, the error wouldn't have happened in a hand written order. (It also wouldn't have happened if the computer system required both name and room number to enter an order.)
The Times editorial is based on a study that appeared last week in the New England Journal of Medicine. (Unfortunately it’s only available online with a subscription). What the editorial doesn’t mention is that the public and physicians are on the same page when it comes to medical errors and their relative importance:
Neither physicians nor the public named medical errors as one of the largest problems in health care today. The problems cited most frequently by physicians were the costs of malpractice insurance and lawsuits (cited by 29 percent of the respondents), the cost of health care (27 percent), and problems with insurance companies and health plans (22 percent). In the survey of the public, the issues cited most frequently were the cost of health care (cited by 38 percent of the respondents) and the cost of prescription drugs (31 percent). Only 5 percent of physicians and 6 percent of the public identified medical errors as one of the most serious problems.
...The majority of both physicians and the public believed that 5000 or fewer deaths in hospitals each year are due to preventable medical errors — a much lower number than either the high or low IOM estimate. A majority of respondents in both surveys thought that one half or fewer of these deaths could have been prevented.
And it’s not only physicians who don’t agree with the solutions endorsed by the Times:
Of the 16 proposed solutions, a majority of physicians thought that 2 would be very effective at reducing the number of medical errors: requiring hospitals to develop systems for preventing medical errors (55 percent) and increasing the number of nurses in hospitals (51 percent). A majority of the respondents in the survey of the public rated eight items as very effective. The top four items were giving physicians more time to spend with their patients (78 percent), requiring hospitals to develop systems for preventing errors (74 percent), providing better training of health professionals (73 percent), and using only physicians trained in intensive care medicine on intensive care units (73 percent).
...Seventy-one percent of physicians thought that an error would be more likely at a hospital that performs a low volume of procedures than at a high-volume center. The public was divided on this issue; about half the respondents thought that an error would be more likely at a low-volume center (49 percent), and the other half thought either that an error would be more likely at a high-volume center (23 percent) or that volume would make no difference (26 percent).... In neither group did a majority of respondents think that limiting certain high-risk procedures to high-volume centers would be a very effective way to reduce medical errors.
The general public did feel that serious medical errors should be openly reported, whereas physicians didn’t. That’s understandable. Physicians are naturally suspiscious of state interference. Just coming to a mutually agreeable definition of what constitutes an error would be difficult. And a state system could prove to be unwieldy and punative. There isn’t a man who walks this earth who doesn’t make mistakes once in a while. But, patients deserve to know about errors. If not on a system-wide basis, at least on an individual basis. When errors are made in their care, the right thing to do is to admit to it, and face the consequences. You’d be surprised at how often those consequences turn out to be forgiveness. posted by Sydney on
12/18/2002 09:37:00 AM
0 comments
Smallpox Martyrs: Glenn Reynolds argues that Americans who opt for smallpox vaccination are doing both us and the world a noble favor. posted by Sydney on
12/18/2002 08:19:00 AM
0 comments
Other Vaccine News: The FDA approved a new pediatric immunization that combines three shots that are now given separately - DTaP, polio, and hepatitis B. The immunization, Pediarix will decrease the number of shots (or “jabs” as the British say) a child gets at a well child visit from four to three. How can that be? Because some of the other shots are already available in a combined form.
At the typical well-child visit at two months of age a child gets these shots - DTaP, polio, Prevnar (for pneumonia) and Hib (for meningitis). At four and six months, they also get a hepatitis B shot, but that already comes in a combination form with the Hib shot. So, the only advantage of the new vaccine is that it combines IPV with DTaP. The disadvantage is that it has a higher incidence of post-immunization fever. The current regimen has a fairly low rate of that, much lower than it was in the old days when the cellular form of pertussis was used for the DTP. I’m not sure it’s worth the trade-off. (And who knows what the price tag will be?) posted by Sydney on
12/17/2002 08:13:00 AM
0 comments
Perfect Storm: Proponents of healthcare reform have taken to characterizing our current state as “a perfect storm.” If we don’t do something quick, the thinking is, we’ll all drown. Insurance premiums are increasing, and those without jobs or who are self-employed can’t get insurance, but the majority of us are still sitting pretty when it comes to health insurance. That's because the majority of us are employed.
Senator Ted Kennedy, though, sees this perfect storm as the perfect chance to once again launch an attempt at socialized medicine. He’s planning to announce his plan in January:
Kennedy's plan, according to Manley, "begins with building on the current health-care system in this country, basing it on an employer mandate for companies with five or more employees."
Employers would be required to subsidize health-insurance premiums at 75 percent, with the employee responsible for 25 percent.
This is just ridiculous. We need to get employers out of the equation. First of all, it isn't "universal" if small businesses (less than five employees) are exempt. That leaves out millions of people right out of the gate. Second of all, employers need to be in the business of their business, not providing government mandated paternalistic cradle to grave benefits for their employers. If Ted Kennedy had ever had to work a day in his life or run a business and make a payroll, he might understand this.
Last Word: Ross at The Bloviator has an excellent introduction to the subtleties of living wills, those documents that are supposed to let your loved ones and physician know what you do and don’t want done to you as you descend into the final days of life. It’s worth a read. Things aren’t as straightforward as you might think:
The problem is, living wills, as generally executed, are very limited in their scope. They are usually restricted to very specific circumstances; namely, when (a) the patient cannot express their own wishes, and (b) the patient is terminal. Part (b) is what usually keeps the Living Will from kicking in. Under Illinois' Living Will Act, a “terminal condition” is an incurable and irreversible condition such that death is imminent and the application of death delaying procedures serves only to prolong the dying process. "Imminent" has been defined by one court as "near at hand; mediate rather than immediate; close rather than touching; impending; on the point of happening; threatening; menacing; perilous." There isn’t a strict time line – i.e., less than 10 days – but one court has said that a week or less would be considered “imminent.” A death delaying procedure means any medical procedure or intervention which, when applied to a qualified patient, in the judgement of the attending physician would serve only to postpone the moment of death.
Keep in mind that this becomes an issue only when the family can't agree among themselves what the intent of the living will is, or when the physician and family can't agree.This is why it’s important to have a heart to heart discussion with both your family - especially the person you’ve designated as the decision maker if you become incompetent, and with your doctor, about just exactly what you have in mind for your final days, and what you consider those final days to be. For some, the final days may be now. They may never, ever, want to be resuscitated, under any circumstances, even though their death isn’t knowingly imminent; even though they're fairly healthy. Others, although in the poorest of health, may want to be resuscitated, but not kept indefinitely on machines, or to forego intervention only if they have a clearly terminal and hopeless condition, like widespread cancer.
This is also a reason that it's important to have a primary care doctor, or generalist, who knows you well, and who is willing to take an active part in all of your care. (Both DB and RangelMD have discussed the important role of the generalist recently.) It’s important to have a physician who can act as your advocate in the hospital, who knows you and your desires, and who can run interference between the specialists and your family (or you).
I’m struggling with this issue with one of my patients, even as I write. He had a stroke a few weeks ago and went to a rehab center to recuperate. While there, he aspirated (something he ate or drank went down the wrong way.) He developed pneumonia. He was taken to the emergency room in severe respiratory distress and ended up on a ventilator. He has more than his fair share of medical problems - heart disease, a history of strokes, poor circulation in his legs - all mostly due to years of diabetes. He has a living will, but he made it clear to me every time we discussed it that he wanted intervention unless there was absolutely no hope. But, I had a hard time conveying that distinction to the intensivist taking care of him. He was upset that he had ended up on the ventilator. I’m still having a hard time getting him to understand that this is what the patient would have wanted. He only sees a guy with endstage diabetes. He hasn't seen him within the context of his family, and his beliefs. He doesn't understand that my patient, as ill as he is, still feels he has a lot of living to do and doesn't want to miss out on any of it if he can help it. posted by Sydney on
12/17/2002 07:24:00 AM
0 comments
Pro-Choice: Tommy Thompson won't, George W. will, but his family won’t. The important thing is that we all be given the opportunity to make the same sort of choices. posted by Sydney on
12/17/2002 07:19:00 AM
0 comments
Monday, December 16, 2002
USA in the BMJ: The British Medical Journal often has news items from the United States that never get much media attention here. Did you know, for example, that Oregon had a board of State Social Protection, responsible for enforcing eugenics laws as recently as 1983?
Until reforms in 1967, sterilization was regularly used by state officials as a condition of release from state institutions or to punish people who acted out. Oregon initially used the eugenics laws to punish homosexuals. Later, state officials tended toward castrations instead of vasectomies. It wasn't until 1983 that the board, then called the State Board of Social Protection, was abolished.
They really are deserving of the moniker People’s Republic of Oregon.
Or, did you know that outgoing president of the American Heart Association was reprimanded by the FDA for irregularities in his research:
The complaint cited examples of records being falsified to alter the duration of chest pain; changes in the records that led to the inclusion of patients who were not eligible for inclusion; patients being included despite being enrolled after the time limits; patients being included when they were receiving drugs that should have excluded them.
Dr Faxon answered the FDA in December 1999,?saying his study's coordinator was responsible for misrepresentation of data and he had no knowledge of the practice. The FDA rejected his response: "We remind you that you are responsible for personally conducting and supervising the clinical investigations since you are the investigator of record. Therefore, we consider your explanation unacceptable."
In April 2000,- the FDA sent Dr Faxon a "Notice of Initiation of Disqualification Proceedings and Opportunity to Explain (NIDPOE)." Few clinical investigators receive such a notice. In 2000, Dr Faxon was one of only six to receive one. In 2001 there were four, and so far this year there have been two.
The research involved comparing aspirin to another drug to see which was better for protecting the heart from further injury after a heart attack. Neither the BMJ, nor the FDA letter (pdf file) identifies the drug. This may not seem like much, but remember that the American Heart Association makes it their business to write guidelines about treatment care. Not long ago, they came under criticism for recommending the use of a clot-buster of dubious effectiveness. Several members of the panel writing the guidelines and the American Heart Association themselves were financially beholden to the company that makes the drug. Knowing that their former president was also involved in dubious research doesn’t do much to boost confidence in them. posted by Sydney on
12/16/2002 08:07:00 AM
0 comments
A publicist from a big agency with corporate clients called on a hunch.
"This might be a long shot," she said. "But this is the hot new disease."
Everybody who is anybody has I.B.S., she said, rattling off names: a comedian, an actress, a celebrity couple. Even John F. Kennedy, whose diagnosis was just made, posthumously.
"Irritable bowel syndrome," the publicist said. Lynda Carter - an actress perhaps best remembered as Wonder Woman in the 1970's - was to be the new celebrity spokeswoman for the syndrome.
John F. Kennedy didn't have irritable bowel syndrome. He had some sort of inflammatory bowel disease - much more serious, poorer prognosis, and many more serious health implications for the rest of the body. Musn't get our celebrity illnesses confused.
Lynda Carter doesn’t have IBS, either, but evidently her mother did. It’s basically a nervous gut. Stress tends to set off the symptoms of diarrhea and gas, and sometimes constipation. It’s never fatal, but it can be uncomfortable and inconvenient. She is, of course, pushing a drug, although she never mentions it by name. She’s on the payroll of Novartis.
As a society we must be reaching the point where we’re no longer impressed by celebrity opinions. They voice them sooften and sostupidly. This may be the unintended benefit of their political activism. One day they won’t have as much influence in other areas, like disease promotion, either. Soon, the majority of the public will think like this man:
Celebrities, he said, often want to raise money for so-called orphan diseases. "And that is wonderful," he said. "But the science may not yet be there to treat a certain form of Alzheimer's in quite the same way it is there to treat, say, diarrhea in third-world Africa."
"You could save a lot of lives with simple vaccinations, with oral rehydration in Africa," he continued. "But the celebrity fund-raisers don't care. It is not wrong to raise that money. But someone on the political or foundation or even university side ought to say, `Thank you, Mr. Celebrity, and you ought to give us a little discretion.' " posted by Sydney on
12/16/2002 07:36:00 AM
0 comments
Insurance Conundrum: Yet more arguments for divorcing health insurance from employment:
When Chip East, 31, of Jersey City left his job as a newspaper photographer in Fayetteville, N.C., four years ago to try his hand at freelancing, he didn't expect to be without health insurance for long. But the policies he found were more than he could afford, and Mr. East is still uninsured.
Last year, in addition to picking up a nasty intestinal parasite and being shot in the leg while on assignment in Israel, Mr. East was found to have skin cancer and had to have two surgeries. Although he plans to sign on with his future wife's group plan after he marries in March, his troubles may not be over. If his intestinal problems or skin cancer recur, he may not be covered for those conditions for up to a year because the break in coverage has been more than 62 days.
The article is really about loopholes in the HIPPA regulations (Health Insurance Privacy and Portability Act) that fail to protect people from losing their insurance when they change jobs. The writer seems to favor a different solution than just selling healthcare directly to people instead of through employers:
Is anyone calling for any revisions to Hipaa (sic) to close these loopholes on pre-existing conditions? If anything, political momentum is moving in the opposite direction — toward less comprehensive coverage and fewer safeguards and protections.
Coverage gaps may be among the least of our worries.
Of course, if insurance companies sold insurance directly to all of us, using the general population as a risk pool, instead of groups of employees, none of those problems would exist. Coverage may be less comprehensive, but health care spending would be more responsible and no one would lose coverage when they lost their job or decided to work for themselves.
CORRECTION: Both the University of South Dakota School of Medicine and I have gotten the acronym wrong for that irksome piece of legislation, correctly called HIPAA - Health Insurance Portability and Accountability Act. I can't speak for the South Dakota Medical School, but I know my error comes from seeing somanyimagesofhippos associated with it. posted by Sydney on
12/16/2002 07:32:00 AM
0 comments
Inspiration:The New York Times Book Review had a review of a book that sounds intriguing. It's the story of a couple who decided to have their baby after prenatal testing diagnosed Down's Syndrome :
The most noteworthy portion of ''Choosing Naia'' centers on the fast-moving three weeks between the diagnosis and the 24-week deadline for a legal abortion in Connecticut, where Tierney and Greg then lived. Their struggle to decide, and, later, their feelings about that decision, underscore the limits of prenatal technology. With Down syndrome, an amniocentesis or a blood test can't tell us how severe the disabilities might be. And no test -- so far -- can reveal a child's temperament or personality, much less how much we will love that child or how that child will change our lives, our priorities and our values.
Antibiotic Resistance Update: The United Kingdom is noticing a trend in the increase in bacteria resistant to commonly used antibiotics. Last week, a Scottish woman died after developing a post-surgical infection caused by a super-resistant strain of Staphylococcus aureus. Also, last week, the British Medical Journal published a study showing that there has been an increase in deaths caused by the more run-of-the-mill resistant variant, methicillin resistant staphylococcus aureus:
A study published yesterday in the British Medical Journal showed that deaths associated with MRSA increased from 7.5 per cent in 1993 to 25 per cent in 1998 in England and Wales. Experts in Scotland have said the trend is being mirrored north of the Border.
MRSA can be treated with the antibiotic vancomycin. The strain that the woman in Scotland had, is resistant to vancomycin. They tested the hospital and its staff for evidence of that particular type of bacteria, but came up empty. It’s likely that it came from the woman’s own skin. Moral of the story: Don’t give in to the temptation to use antibiotics for those winter sniffles. It only increases the risk of growing these resistant bugs. posted by Sydney on
12/15/2002 12:38:00 PM
0 comments
NOTE: The post below on The New Republic's article about the pharmaceutical industry had some bad links. They're fixed now. I shouldn't try to blog and make waffles at the same time. posted by Sydney on
12/15/2002 12:09:00 PM
0 comments
Profits Where No Pleasure's Taken: The December 16 issue of The New Republic has a novella-length critique of the pharmaceutical industry (unfortunately not available on the internet) by two former editors of The New England Journal of Medicine, Marcia Angell and Arnold S. Relman. I don’t feel qualified to comment on some of it, especially the assertions about the economics and the process of developing and testing drugs. I’ll leave that to other more qualified people. But, it does deserve a second look from a medical perspective.
It is a sweeping indictment of the drug industry. Its central argument is that drug companies depend on government-funded research to develop drugs and then make obscene profits by bringing the final product to market. I’m not sure that’s a valid criticism. Surely, the drug companies have some researchers in house, people, like Derek Lowe, who spend their working days trying to develop new drugs. The article offers as proof or their assertion the results of a study published in Health Affairs:
The study reported that in 1998 only about 15 percent of the scientific articles cited in patent applications for clinical medicine came from industry research, while 54 percent came from academic centers, 13 percent from government, and the rest from various other public and nonprofit institutions.
But how many of those articles from academic centers encompassed research funded by grants from the pharmaceutical industry? As the authors note elsewhere in their manifesto, these days the distinction between industry and academia is hopelessly blurred. It’s hard to find a researcher who doesn’t have some ties to the pharmaceutical industry, and it’s even hard to find research that isn’t funded at least in part by them. So hard, in fact, that The New England Journal announced not long ago that they would no longer bar writers of review articles who had any connection to pharmaceutical or biotech companies involved in the topic of the article. They couldn’t find any experts without ties.
Angell and Relman detail the drug companies’ successful efforts to end-run the patent system, including copy-cat drugs and dubious patent claims and lawsuits against generic companies. They fail to mention the influence of “pharmaceutical benefits management” companies that are owned by drug companies. These are entities paid by insurance companies to manage the drug benefits of their beneficiaries. They’re often, as in the case of Merck-Medco, owned by the drug companies. Merck-Medco is just plain Medco now, but Merck has still held them to a promise to push Merck drugs. They have no interest in allowing the cheapest, most effective drugs for their beneficiaries, but every interest in pushing Merck products. So, when a new copy-cat drug comes out to dodge a patent expiration, they send out notices advising physicians to switch patients from the old drug to the new. They say the new drug is the "preferred drug." They don’t care about cost or effectiveness. Their “formulary” is designed to increase market share for their parent drug company.
The article’s greatest strength, though, is in its details of the marketing of drugs to doctors, and in the medical profession’s willing acquiesence:
The atmosphere at many large medical meetings resembles a bazaar, dominated by the presence of garish drug company exhibits and friendly salespeople eager to ply physicians with samples, gifts, and services while they pitch their company’s drugs. In the exhibit areas adjacent to the meeting rooms, physicians wander through a carnival-like scene. Many carry large canvas bags, bearing drug company logos, stuffed with goodies.
That, sadly, is an accurate description of most large medical meetings. It’s a disgusting sight. Unfortunately, it’s also true that a lot of physicians, and most medical societies have no interest in changing that behavior. Physicians have come to think of free handouts as a perq of the job. Medical societies and professional organizations have come to rely on drug company “sponsors” to finance their educational meetings. As a profession, we’ve pretty much prostituted ourselves to the pharmaceutical industry.
Angell and Relman correctly include the medical profession in their call for reform. There is too much collusion in research and too much marketing to physicians. But they fail to mention the role that medical journals and their editors play in this, too. It’s the journals that publish the studies with biased findings. The journal editors who allow authors of papers to cast their results in the most positive of lights with misleading statistics. Who make no distinction between statistical significance and clinical significance. Who send out press releases to the media to hype the research of the week - press releases that parrot the optimistic conclusions of the authors. That media attention is just as influential in hyping a new treatment or drug, to both doctors and patients, as any marketing campaign. (For more on this, click here.)
The authors express little hope that things will change, citing a Republican Congress as a likely road block to reform. This is odd, given that they cite plenty of examples of Democrats who have been just as culpable in laws favoring drug companies, and they note that the pharmaceutical industry gives liberally to politicians of both parties. The current state of affairs didn't arise de novo over the past two years of a Republican Administration. A lot of it evolved during the 1990's, during the reign of a Democrat.
The reason they despair of the current Republican leadership is that their ultimate solution isn't aimed just at solving the problems of high drug prices. Their ultimate solution dove-tails nicely with Marcia Angell's other project - campaigning for a national healthcare system. At the very end of their very long treatise, they call for a single-payer system, arguing that one payer could negotiate better drug prices than our current multi-faceted system. Such a system would certainly lower drug prices, but it would also force a lot of drug companies if not completely out of business, at least out of the business of making new drugs.
Single-payer systems give all the advantage to the payer, and none to the seller. It's a reverse monopoly, and like all monopolies, it's no good. It would be far better to allow market forces to bring down the price of drugs by having the people who use them bear the responsibility for buying them - especially in the cases of those chronic conditions with a wide choice of drugs to treat them - like arthritits, diabetes, and hypertension. It would be far better to legislate reform that addresses patent system abuses so that competition within the industry can be increased. It would be better to eliminate marketing to consumers and doctors. Let a drug be evaluated and adopted on its merits rather than the company sales pitch. Then, the money that’s being used to feed doctors could be used to feed research chemists. Finally, we need reform of the leadership of our medical journals. Editors need to take more responsibility for the spin their authors put on their papers, and they need to stop using that spin for their own ends - keeping their journals in the public eye. Surely, two former editors of The New England Journal of Medicine could do something about that.
NOTE: I fixed the broken links that appeared here earlier.
UPDATE: The BMJ has taken the lead in transparency of competing interests for medical journals. They've posted their competing interests on the internet. posted by Sydney on
12/15/2002 07:55:00 AM
0 comments




{kind=link}
{kind=link}